Mindell Jennifer S, Giampaoli Simona, Goesswald Antje, Kamtsiuris Panagiotis, Mann Charlotte, Männistö Satu, Morgan Karen, Shelton Nicola J, Verschuren W M Monique, Tolonen Hanna
Research Department of Epidemiology & Public Health, UCL, 1-19 Torrington Place, London, WC1E 6BT, UK.
Istituto Superiore di Sanità, Viale Regina Elena n. 299, Rome, Italy.
BMC Med Res Methodol. 2015 Oct 5;15:78. doi: 10.1186/s12874-015-0072-4.
Health examination surveys (HESs), carried out in Europe since the 1950's, provide valuable information about the general population's health for health monitoring, policy making, and research. Survey participation rates, important for representativeness, have been falling. International comparisons are hampered by differing exclusion criteria and definitions for non-response.
Information was collected about seven national HESs in Europe conducted in 2007-2012. These surveys can be classified into household and individual-based surveys, depending on the sampling frames used. Participation rates of randomly selected adult samples were calculated for four survey modules using standardised definitions and compared by sex, age-group, geographical areas within countries, and over time, where possible.
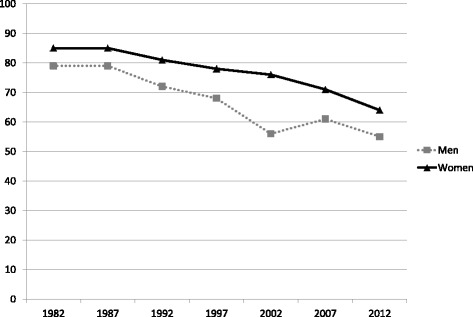
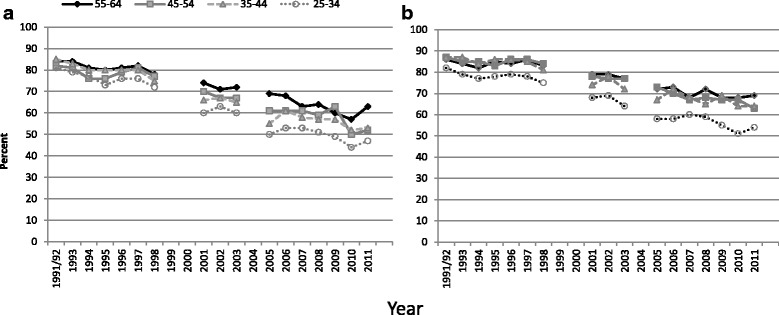
All surveys covered residents not just citizens; three countries excluded those in institutions. In two surveys, physical examinations and blood sample collection were conducted at the participants' home; the others occurred at examination clinics. Recruitment processes varied considerably between surveys. Monetary incentives were used in four surveys. Initial participation rates aged 35-64 were 45% in the Netherlands (phase II), 54% in Germany (new and previous participants combined), 55% in Italy, and 65% in Finland. In Ireland, England and Scotland, household participation rates were 66%, 66% and 63% respectively. Participation rates were generally higher in women and increased with age. Almost all participants attending an examination centre agreed to all modules but surveys conducted in the participants' home had falling responses to each stage. Participation rates in most primate cities were substantially lower than the national average. Age-standardized response rates to blood pressure measurement among those aged 35-64 in Finland, Germany and England fell by 0.7-1.5 percentage points p.a. between 1998-2002 and 2010-2012. Longer trends in some countries show a more marked fall.
The coverage of the general population in these seven national HESs was good, based on the sampling frames used and the sample sizes. Pre-notification and reminders were used effectively in those with highest participation rates. Participation rates varied by age, sex, geographical area, and survey design. They have fallen in most countries; the Netherlands data shows that they can be maintained at higher levels but at much higher cost.
自20世纪50年代以来在欧洲开展的健康检查调查(HESs),为健康监测、政策制定和研究提供了有关普通人群健康状况的宝贵信息。对于代表性很重要的调查参与率一直在下降。不同的排除标准和无应答定义阻碍了国际间的比较。
收集了2007年至2012年在欧洲开展的七项国家健康检查调查的信息。根据所使用的抽样框架,这些调查可分为基于家庭和基于个人的调查。使用标准化定义计算了四个调查模块中随机抽取的成年样本的参与率,并按性别、年龄组、国家内的地理区域以及在可能的情况下按时间进行了比较。
所有调查涵盖的是居民而非仅仅是公民;三个国家将机构中的人员排除在外。在两项调查中,体格检查和血样采集在参与者家中进行;其他调查在检查诊所进行。不同调查之间的招募过程差异很大。四项调查使用了金钱激励措施。35至64岁人群的初始参与率在荷兰(第二阶段)为45%,在德国(新参与者和先前参与者合并)为54%,在意大利为5