Barakat M F, McDonald H I, Collier T J, Smeeth L, Nitsch D, Quint J K
Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK.
Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK ; Department of Respiratory Epidemiology, Occupational Medicine and Public Health, National Heart and Lung Institute, Imperial College London, London, UK.
Int J Chron Obstruct Pulmon Dis. 2015 Sep 28;10:2067-77. doi: 10.2147/COPD.S88759. eCollection 2015.
While acute kidney injury (AKI) alone is associated with increased mortality, the incidence of hospital admission with AKI among stable and exacerbating COPD patients and the effect of concurrent AKI at COPD exacerbation on mortality is not known.
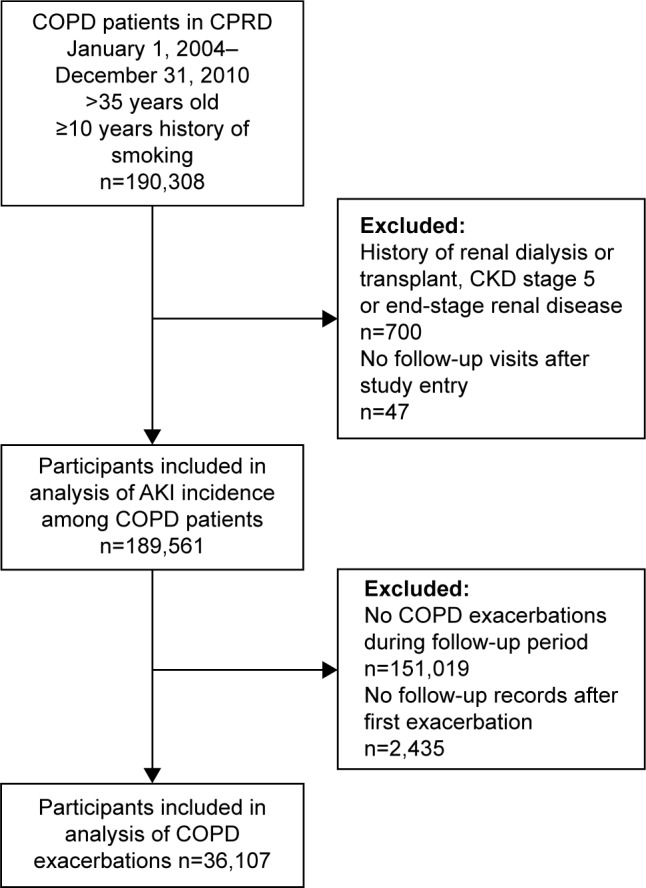
A total of 189,561 individuals with COPD were identified from the Clinical Practice Research Datalink. Using Poisson and logistic regressions, we explored which factors predicted admission for AKI (identified in Hospital Episode Statistics) in this COPD cohort and concomitant AKI at a hospitalization for COPD exacerbation. Using survival analysis, we investigated the effect of concurrent AKI at exacerbation on mortality (n=36,107) and identified confounding factors.
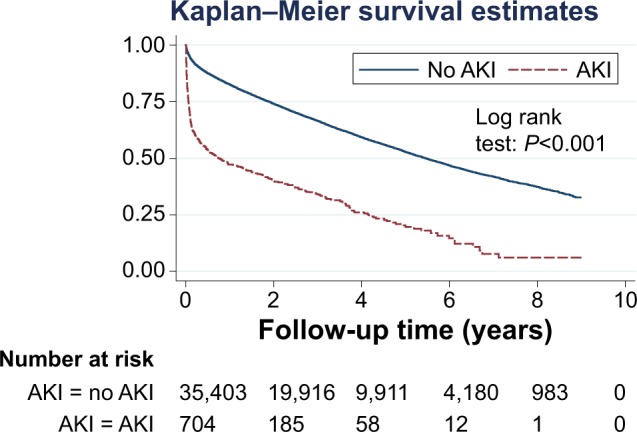
The incidence of AKI in the total COPD cohort was 128/100,000 person-years. The prevalence of concomitant AKI at exacerbation was 1.9%, and the mortality rate in patients with AKI at exacerbation was 521/1,000 person-years. Male sex, older age, and lower glomerular filtration rate predicted higher risk of AKI or death. There was a 1.80 fold (95% confidence interval: 1.61, 2.03) increase in adjusted mortality within the first 6 months post COPD exacerbation in patients suffering from AKI and COPD exacerbation compared to those who were AKI free.
In comparison to previous studies on general populations and hospitalizations, the incidence and prevalence of AKI is relatively high in COPD patients. Coexisting AKI at exacerbation is prognostic of poor outcome.
虽然单纯急性肾损伤(AKI)与死亡率增加相关,但稳定期和加重期慢性阻塞性肺疾病(COPD)患者因AKI住院的发生率以及COPD加重期并发AKI对死亡率的影响尚不清楚。
从临床实践研究数据链中识别出总共189,561例COPD患者。我们使用泊松回归和逻辑回归,探讨了哪些因素可预测该COPD队列中因AKI住院(在医院事件统计中确定)以及COPD加重期住院时并发AKI的情况。我们使用生存分析,研究了加重期并发AKI对死亡率(n = 36,107)的影响,并确定了混杂因素。
整个COPD队列中AKI的发生率为128/100,000人年。加重期并发AKI的患病率为1.9%,加重期患有AKI的患者死亡率为521/1,000人年。男性、老年和较低的肾小球滤过率预示着AKI或死亡的风险更高。与无AKI的患者相比,患有AKI且COPD加重的患者在COPD加重后前6个月内调整后的死亡率增加了1.80倍(95%置信区间:1.61, 2.03)。
与先前关于一般人群和住院情况的研究相比,COPD患者中AKI的发生率和患病率相对较高。加重期并存AKI提示预后不良。