Huang Yi, Huang Hai, Pan Xiu-Wu, Xu Dan-Feng, Cui Xin-Gang, Chen Jie, Hong Yi, Gao Yi, Yin Lei, Ye Jian-Qing, Li Lin
Department of Urinary Surgery of Changzheng Hospital, Second Military Medical University, Shanghai 200003, China.
Urology Research Center of the Chinese People's Liberation Army, Changzheng Hospital, Second Military Medical University, Shanghai 200003, China.
Asian J Androl. 2016 Sep-Oct;18(5):780-5. doi: 10.4103/1008-682X.156636.
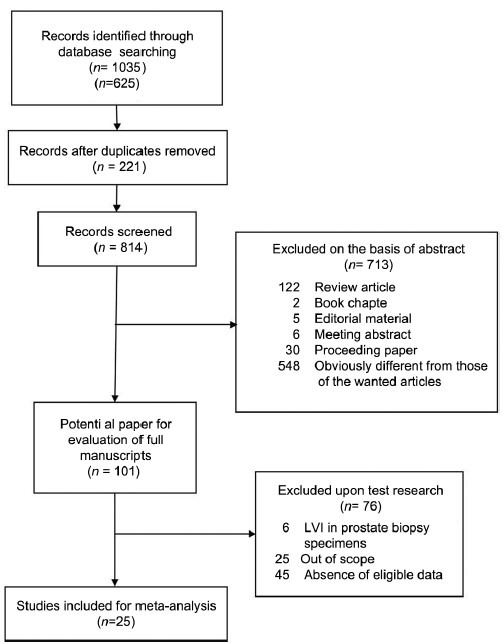
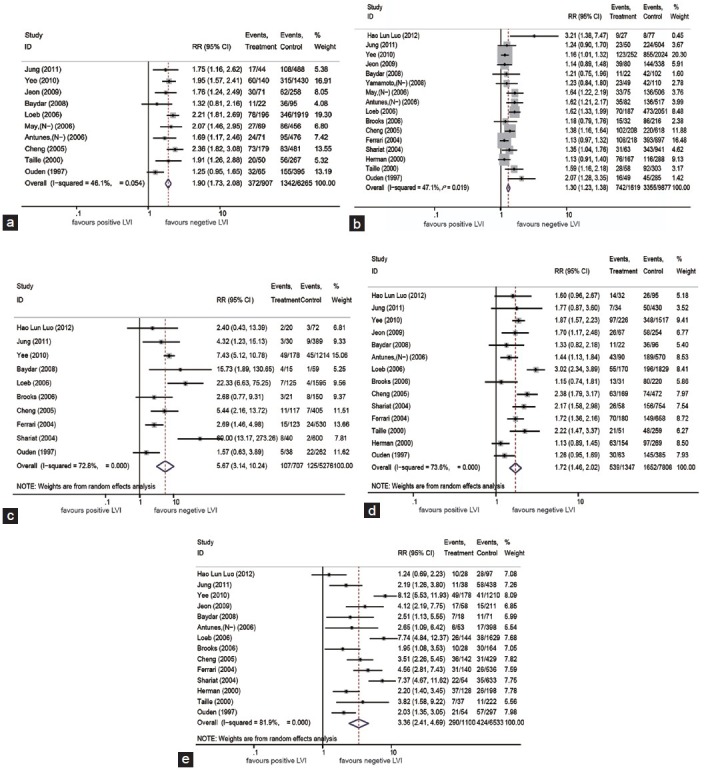
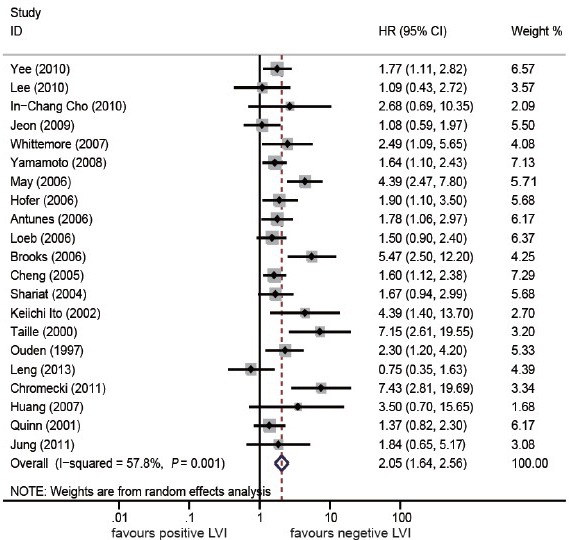
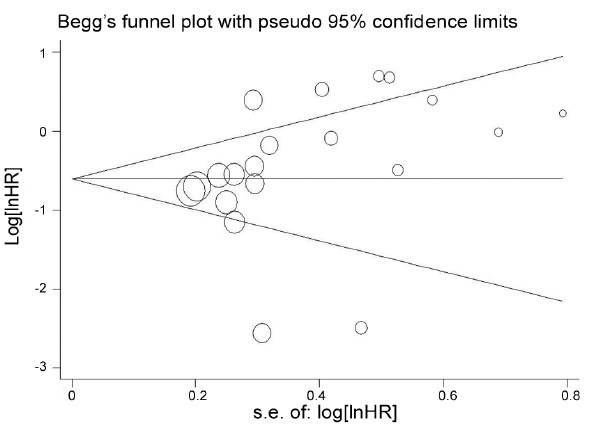
To systematically evaluate the prognostic value of lymphovascular invasion (LVI) in radical prostatectomy (RP) by a meta-analysis based on the published literature. To identify relevant studies, PubMed, Cochrane Library, and Web of Science database were searched from 1966 to May 2014. Finally, 25 studies (9503 patients) were included. LVI was found in 12.2% (1156/9503) of the RP specimens. LVI was found to be correlated with higher pathological tumor stages (greater than pT3 stage) (risk ratio [RR] 1.90, 95% confidence interval [CI] 1.73-2.08, P< 0.00001), higher Gleason scores (greater than GS = 7) (RR 1.30, 95% CI 1.23-1.38, P< 0.00001), positive pathological node (pN) status (RR 5.67, 95% CI 3.14-10.24, P< 0.00001), extracapsular extension (RR 1.72, 95% CI 1.46-2.02, P< 0.00001), and seminal vesicle involvement (RR 3.36, 95% CI 2.41-4.70, P< 0.00001). The pooled hazard ratio (HR) was statistically significant for Biochemical Recurrence-Free (BCR-free) probability (HR 2.05, 95% CI 1.64-2.56; Z = 6.30, P< 0.00001). Sensitivity analysis showed that the pooled HR and 95% CI were not significantly altered by the omission of any single study. Begg's Funnel plots showed no significant publication bias (P = 0.112). In conclusion, LVI exhibited a detrimental effect on the BCR-Free probability and clinicopathological features in RP specimens, and may prove to be an independent prognostic factor of BCR.
通过基于已发表文献的荟萃分析,系统评价前列腺癌根治术(RP)中淋巴管侵犯(LVI)的预后价值。为确定相关研究,检索了1966年至2014年5月的PubMed、Cochrane图书馆和科学网数据库。最终纳入25项研究(9503例患者)。在RP标本中发现LVI的比例为12.2%(1156/9503)。发现LVI与更高的病理肿瘤分期(大于pT3期)相关(风险比[RR]1.90,95%置信区间[CI]1.73 - 2.08,P<0.00001)、更高的Gleason评分(大于GS = 7)(RR 1.30,95%CI 1.23 - 1.38,P<0.00001)、阳性病理淋巴结(pN)状态(RR 5.67,95%CI 3.14 - 10.24,P<0.00001)、包膜外侵犯(RR 1.72,95%CI 1.46 - 2.02,P<0.00001)和精囊受累(RR 3.36,95%CI 2.41 - 4.7, P<0.00001)。对于无生化复发(BCR-free)概率,合并风险比(HR)具有统计学意义(HR 2.05,95%CI 1.64 - 2.56;Z = 6.30,P<0.00001)。敏感性分析表明,剔除任何一项研究后,合并HR和95%CI均无显著改变。Begg漏斗图显示无显著发表偏倚(P = 0.112)。总之,LVI对RP标本的无BCR概率和临床病理特征有不利影响,可能是BCR的独立预后因素。