Rahman Rubayat, Schmaltz Chester, Jackson Christian S, Simoes Eduardo J, Jackson-Thompson Jeannette, Ibdah Jamal A
Division of Gastroenterology and Hepatology, University of Missouri School of Medicine, One Hospital Drive, CE 405, Columbia, Missouri, 65212.
Missouri Cancer Registry and Research Center, University of Missouri at Columbia, 401 Clark Hall, Columbia, Missouri, 65211.
Cancer Med. 2015 Dec;4(12):1863-70. doi: 10.1002/cam4.560. Epub 2015 Oct 16.
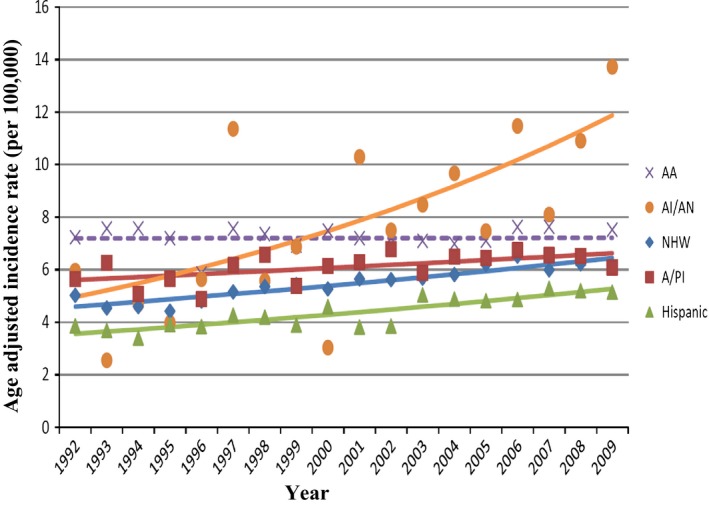
Colorectal cancer (CRC) is the second most common cause of cancer death in USA. We analyzed CRC disparities in African Americans, Hispanics, Asians/Pacific Islanders, and American Indians/Alaska Natives compared to non-Hispanic Whites. Current guidelines recommend screening for CRC beginning at age 50. Using SEER (Surveillance, Epidemiology, and End Results) database 1973-2009 and North American Association of Central Cancer Registries (NAACCR) 1995-2009 dataset, we performed frequency and rate analysis on colorectal cancer demographics and incidence based on race/ethnicity. We also used the SEER database to analyze stage, grade, and survival based on race/ethnicity. Utilizing SEER database, the median age of CRC diagnosis is significantly less in Hispanics (66 years), Asians/Pacific Islanders (68 years), American Indians/Alaska Natives (64 years), and African Americans (64 years) compared to non-Hispanic whites (72 years). Twelve percent of Asians/Pacific Islanders, 15.4% Hispanics, 16.5% American Indians/Alaska Natives, and 11.9% African Americans with CRC are diagnosed at age <50 years compared to only 6.7% in non-Hispanic Whites (P < 0.0001). Minority groups have more advanced stages at diagnosis compared to non-Hispanic Whites. Trend analysis showed age-adjusted incidence rates of CRC diagnosed under the age of 50 years have significantly increased in all racial and ethnic groups but are stable in African Americans. These results were confirmed through analysis of NAACCR 1995-2009 dataset covering nearly the entire USA. A significantly higher proportion of minority groups in USA with CRC are diagnosed before age 50 compared to non-Hispanic Whites, documenting that these minority groups are at higher risk for early CRC. Further studies are needed to identify the causes and risk factors responsible for young onset CRC among minority groups and to develop intervention strategies including earlier CRC screening, among others.
结直肠癌(CRC)是美国癌症死亡的第二大常见原因。我们分析了非西班牙裔白人相比,非裔美国人、西班牙裔、亚裔/太平洋岛民和美国印第安人/阿拉斯加原住民中的结直肠癌差异。当前指南建议从50岁开始进行结直肠癌筛查。利用1973 - 2009年的监测、流行病学和最终结果(SEER)数据库以及1995 - 2009年北美中央癌症登记协会(NAACCR)数据集,我们基于种族/族裔对结直肠癌人口统计学和发病率进行了频率和率分析。我们还使用SEER数据库分析了基于种族/族裔的分期、分级和生存率。利用SEER数据库,与非西班牙裔白人(72岁)相比,西班牙裔(66岁)、亚裔/太平洋岛民(68岁)、美国印第安人/阿拉斯加原住民(64岁)和非裔美国人(64岁)的结直肠癌诊断中位年龄显著更低。结直肠癌患者中,12%的亚裔/太平洋岛民、15.4%的西班牙裔、16.5%的美国印第安人/阿拉斯加原住民和11.9%的非裔美国人在50岁之前被诊断,而非西班牙裔白人中只有6.7%(P < 0.0001)。与非西班牙裔白人相比,少数族裔在诊断时处于更晚期阶段。趋势分析表明,所有种族和族裔群体中50岁以下诊断的结直肠癌年龄调整发病率均显著增加,但非裔美国人保持稳定。通过对覆盖几乎整个美国的NAACCR 1995 - 2009数据集的分析证实了这些结果。与非西班牙裔白人相比,美国患有结直肠癌的少数族裔群体中在50岁之前被诊断的比例显著更高,证明这些少数族裔群体患早期结直肠癌的风险更高。需要进一步研究以确定少数族裔群体中早发性结直肠癌的原因和风险因素,并制定包括更早的结直肠癌筛查等干预策略。