Chowdhary Neerja, Anand Arpita, Dimidjian Sona, Shinde Sachin, Weobong Benedict, Balaji Madhumitha, Hollon Steven D, Rahman Atif, Wilson G Terence, Verdeli Helena, Araya Ricardo, King Michael, Jordans Mark J D, Fairburn Christopher, Kirkwood Betty, Patel Vikram
Neerja Chowdhary, MD, Sangath, Goa, India and London School of Hygiene & Tropical Medicine, London, UK; Arpita Anand, MSc, MA, Sangath, Goa, India; Sona Dimidjian, PhD, University of Boulder, Boulder, Colorado, USA; Sachin Shinde, MPA, Sangath, Goa, India; Benedict Weobong, PhD, Sangath, Goa, India and London School of Hygiene & Tropical Medicine, London, UK; Madhumitha Balaji, MSc, Sangath, Goa, India; Steve D. Hollon, PhD, Vanderbilt University, Nashville, Tennessee, USA; Atif Rahman, PhD, University of Liverpool, Liverpool, UK; G. Terence Wilson, PhD, Rutgers University, New Brunswick, New Jersey, USA; Helena Verdeli, PhD, Teachers College, Columbia University, New York, USA; Ricardo Araya, PhD, London School of Hygiene & Tropical Medicine, London, UK; Michael King, PhD, University College, London, UK; Mark J. D. Jordans, PhD, King's College, London, UK; Christopher Fairburn, PhD, Oxford University, Oxford, UK; Betty Kirkwood, PhD, London School of Hygiene & Tropical Medicine, London, UK; Vikram Patel, FMedSi, Sangath, Goa, Centre for Chronic Conditions and Injuries, Public Health Foundation of India, New Delhi, India and London School of Hygiene & Tropical Medicine, London, UK.
Neerja Chowdhary, MD, Sangath, Goa, India and London School of Hygiene & Tropical Medicine, London, UK; Arpita Anand, MSc, MA, Sangath, Goa, India; Sona Dimidjian, PhD, University of Boulder, Boulder, Colorado, USA; Sachin Shinde, MPA, Sangath, Goa, India; Benedict Weobong, PhD, Sangath, Goa, India and London School of Hygiene & Tropical Medicine, London, UK; Madhumitha Balaji, MSc, Sangath, Goa, India; Steve D. Hollon, PhD, Vanderbilt University, Nashville, Tennessee, USA; Atif Rahman, PhD, University of Liverpool, Liverpool, UK; G. Terence Wilson, PhD, Rutgers University, New Brunswick, New Jersey, USA; Helena Verdeli, PhD, Teachers College, Columbia University, New York, USA; Ricardo Araya, PhD, London School of Hygiene & Tropical Medicine, London, UK; Michael King, PhD, University College, London, UK; Mark J. D. Jordans, PhD, King's College, London, UK; Christopher Fairburn, PhD, Oxford University, Oxford, UK; Betty Kirkwood, PhD, London School of Hygiene & Tropical Medicine, London, UK; Vikram Patel, FMedSi, Sangath, Goa, Centre for Chronic Conditions and Injuries, Public Health Foundation of India, New Delhi, India and London School of Hygiene & Tropical Medicine, London, UK
Br J Psychiatry. 2016 Apr;208(4):381-8. doi: 10.1192/bjp.bp.114.161075. Epub 2015 Oct 22.
Reducing the global treatment gap for mental disorders requires treatments that are economical, effective and culturally appropriate.
To describe a systematic approach to the development of a brief psychological treatment for patients with severe depression delivered by lay counsellors in primary healthcare.
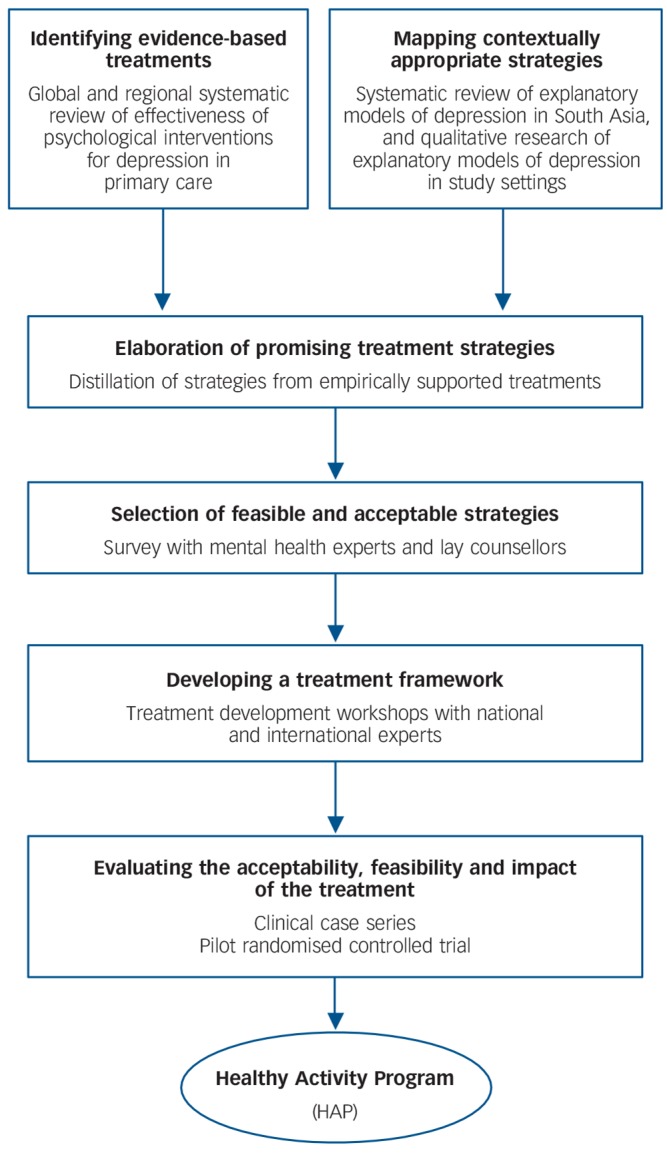
The treatment was developed in three stages using a variety of methods: (a) identifying potential strategies; (b) developing a theoretical framework; and (c) evaluating the acceptability, feasibility and effectiveness of the psychological treatment.
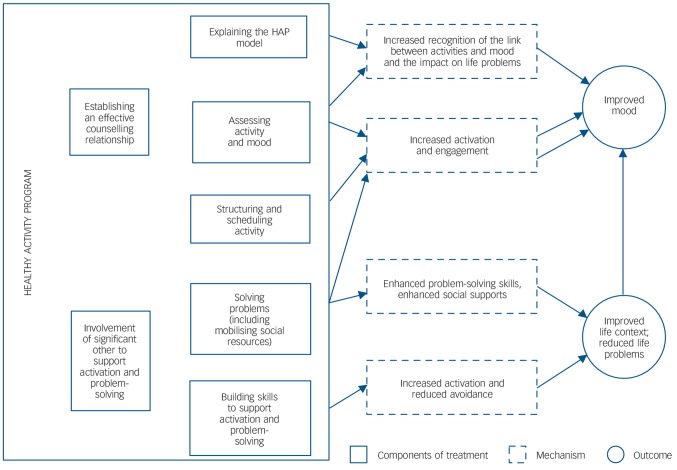
The Healthy Activity Program (HAP) is delivered over 6-8 sessions and consists of behavioral activation as the core psychological framework with added emphasis on strategies such as problem-solving and activation of social networks. Key elements to improve acceptability and feasibility are also included. In an intention-to-treat analysis of a pilot randomised controlled trial (55 participants), the prevalence of depression (Beck Depression Inventory II ⩾19) after 2 months was lower in the HAP than the control arm (adjusted risk ratio = 0.55, 95% CI 0.32-0.94,P= 0.01).
Our systematic approach to the development of psychological treatments could be extended to other mental disorders. HAP is an acceptable and effective brief psychological treatment for severe depression delivered by lay counsellors in primary care.
缩小全球精神障碍治疗差距需要经济、有效且符合文化背景的治疗方法。
描述一种系统方法,用于开发由初级医疗保健中的非专业咨询师为重度抑郁症患者提供的简短心理治疗。
该治疗分三个阶段采用多种方法开发:(a) 确定潜在策略;(b) 构建理论框架;(c) 评估心理治疗的可接受性、可行性和有效性。
健康活动计划(HAP)为期6 - 8节课程,以行为激活为核心心理框架,特别强调解决问题和激活社交网络等策略。还包括提高可接受性和可行性的关键要素。在一项试点随机对照试验(55名参与者)的意向性分析中,HAP组在2个月后抑郁症患病率(贝克抑郁量表II ⩾19)低于对照组(调整风险比 = 0.55,95% CI 0.32 - 0.94,P = 0.01)。
我们开发心理治疗的系统方法可扩展到其他精神障碍。HAP是初级保健中非专业咨询师为重度抑郁症提供的一种可接受且有效的简短心理治疗。