Weobong Benedict, Weiss Helen A, McDaid David, Singla Daisy R, Hollon Steven D, Nadkarni Abhijit, Park A-La, Bhat Bhargav, Katti Basavraj, Anand Arpita, Dimidjian Sona, Araya Ricardo, King Michael, Vijayakumar Lakshmi, Wilson G Terence, Velleman Richard, Kirkwood Betty R, Fairburn Christopher G, Patel Vikram
Centre for Global Mental Health, Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Sangath, Socorro, Goa, India.
PLoS Med. 2017 Sep 12;14(9):e1002385. doi: 10.1371/journal.pmed.1002385. eCollection 2017 Sep.
The Healthy Activity Programme (HAP), a brief behavioural intervention delivered by lay counsellors, enhanced remission over 3 months among primary care attendees with depression in peri-urban and rural settings in India. We evaluated the sustainability of the effects after treatment termination, the cost-effectiveness of HAP over 12 months, and the effects of the hypothesized mediator of activation on clinical outcomes.
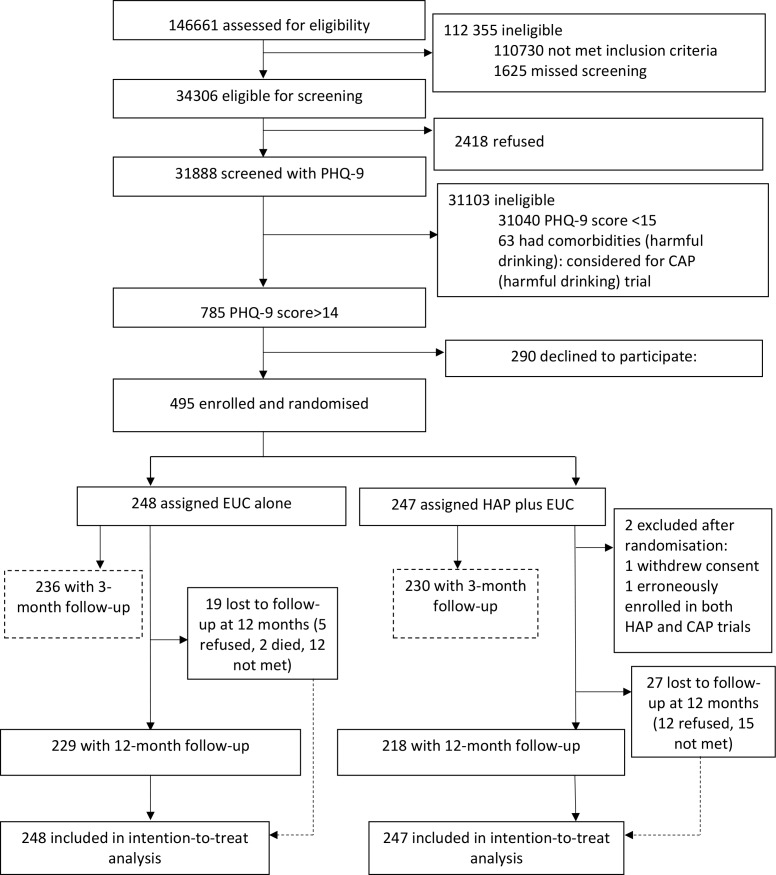
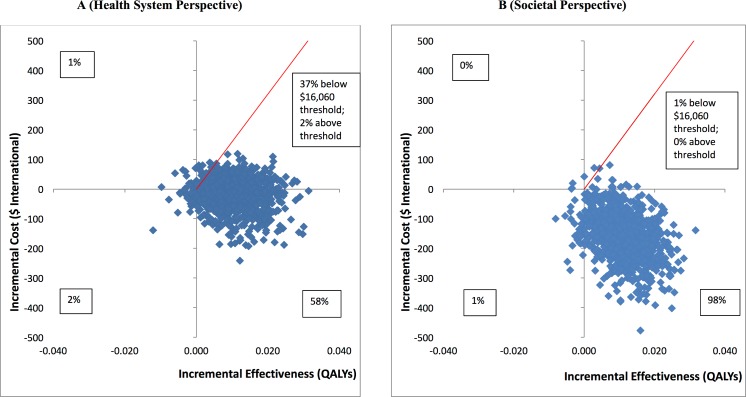
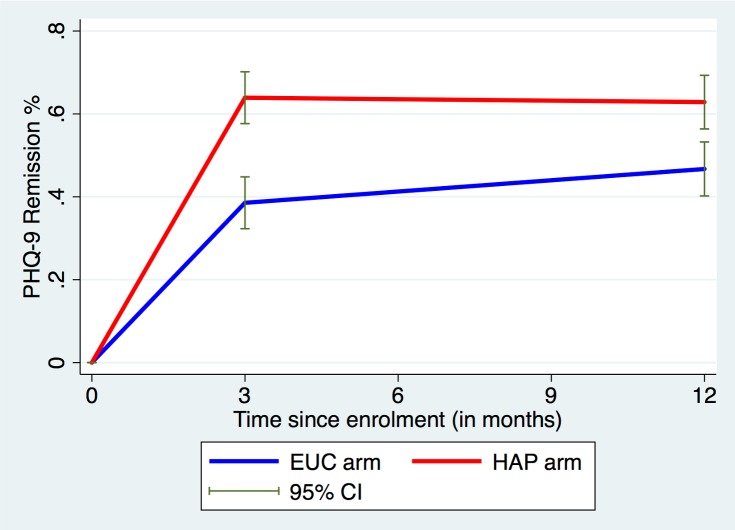
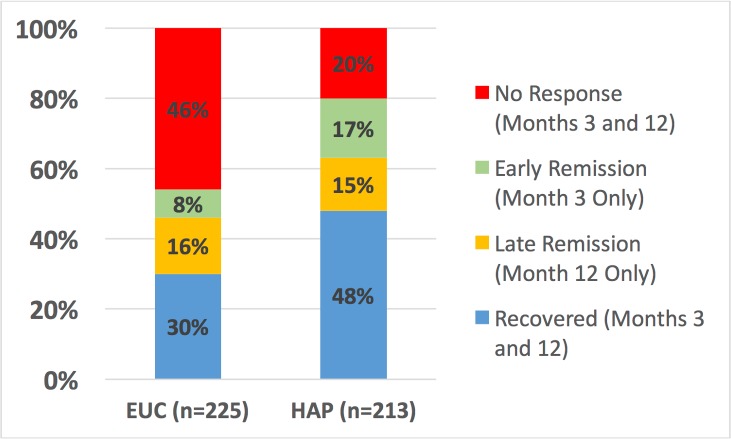
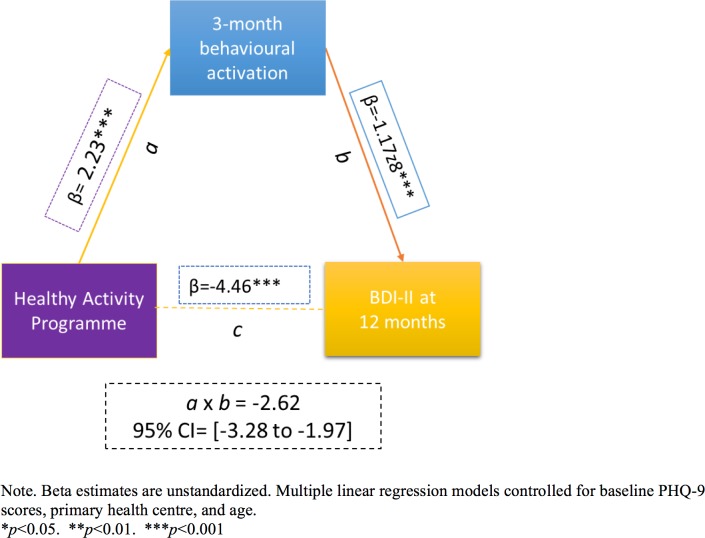
Primary care attendees aged 18-65 years screened with moderately severe to severe depression on the Patient Health Questionnaire 9 (PHQ-9) were randomised to either HAP plus enhanced usual care (EUC) (n = 247) or EUC alone (n = 248), of whom 95% completed assessments at 3 months, and 91% at 12 months. Primary outcomes were severity on the Beck Depression Inventory-II (BDI-II) and remission on the PHQ-9. HAP participants maintained the gains they showed at the end of treatment through the 12-month follow-up (difference in mean BDI-II score between 3 and 12 months = -0.34; 95% CI -2.37, 1.69; p = 0.74), with lower symptom severity scores than participants who received EUC alone (adjusted mean difference in BDI-II score = -4.45; 95% CI -7.26, -1.63; p = 0.002) and higher rates of remission (adjusted prevalence ratio [aPR] = 1.36; 95% CI 1.15, 1.61; p < 0.009). They also fared better on most secondary outcomes, including recovery (aPR = 1.98; 95% CI 1.29, 3.03; p = 0.002), any response over time (aPR = 1.45; 95% CI 1.27, 1.66; p < 0.001), higher likelihood of reporting a minimal clinically important difference (aPR = 1.42; 95% CI 1.17, 1.71; p < 0.001), and lower likelihood of reporting suicidal behaviour (aPR = 0.71; 95% CI 0.51, 1.01; p = 0.06). HAP plus EUC also had a marginal effect on WHO Disability Assessment Schedule score at 12 months (aPR = -1.58; 95% CI -3.33, 0.17; p = 0.08); other outcomes (days unable to work, intimate partner violence toward females) did not statistically significantly differ between the two arms. Economic analyses indicated that HAP plus EUC was dominant over EUC alone, with lower costs and better outcomes; uncertainty analysis showed that from this health system perspective there was a 95% chance of HAP being cost-effective, given a willingness to pay threshold of Intl$16,060-equivalent to GDP per capita in Goa-per quality-adjusted life year gained. Patient-reported behavioural activation level at 3 months mediated the effect of the HAP intervention on the 12-month depression score (β = -2.62; 95% CI -3.28, -1.97; p < 0.001). Serious adverse events were infrequent, and prevalence was similar by arm. We were unable to assess possible episodes of remission and relapse that may have occurred between our outcome assessment time points of 3 and 12 months after randomisation. We did not account for or evaluate the effect of mediators other than behavioural activation.
HAP's superiority over EUC at the end of treatment was largely stable over time and was mediated by patient activation. HAP provides better outcomes at lower costs from a perspective covering publicly funded healthcare services and productivity impacts on patients and their families.
ISRCTN registry ISRCTN95149997.
健康活动计划(HAP)是一项由非专业咨询师提供的简短行为干预措施,在印度城乡结合部和农村地区的初级保健就诊者中,该计划在3个月内提高了抑郁症患者的缓解率。我们评估了治疗终止后效果的可持续性、HAP在12个月内的成本效益,以及假设的激活调节因子对临床结局的影响。
年龄在18 - 65岁、通过患者健康问卷9(PHQ - 9)筛查为中度至重度抑郁症的初级保健就诊者被随机分为HAP加强化常规护理(EUC)组(n = 247)或单独EUC组(n = 248),其中95%的参与者在3个月时完成评估,91%在12个月时完成评估。主要结局指标为贝克抑郁量表第二版(BDI - II)的严重程度和PHQ - 9的缓解情况。HAP参与者在治疗结束后至12个月的随访期间保持了治疗结束时的改善(3个月和12个月之间BDI - II平均得分差异 = -0.34;95%置信区间 -2.37,1.69;p = 0.74),其症状严重程度得分低于仅接受EUC的参与者(BDI - II得分的调整平均差异 = -4.45;95%置信区间 -7.26,-1.63;p = 0.002),缓解率更高(调整患病率比[aPR] = 1.36;95%置信区间1.15,1.61;p < 0.009)。在大多数次要结局指标上,他们的表现也更好,包括康复(aPR = 1.98;95%置信区间1.29,3.03;p = 0.002)、随时间的任何反应(aPR = 1.45;95%置信区间1.27,1.66;p < 0.001)、报告最小临床重要差异的可能性更高(aPR = 1.42;95%置信区间1.17,1.71;p < 0.001),以及报告自杀行为的可能性更低(aPR = 0.71;95%置信区间0.51,1.01;p = 0.06)。HAP加EUC在12个月时对世界卫生组织残疾评估量表得分也有边际效应(aPR = -1.58;95%置信区间 -3.33,0.17;p = 0.08);两组在其他结局指标(无法工作的天数、亲密伴侣对女性的暴力行为)上无统计学显著差异。经济分析表明,HAP加EUC相对于单独的EUC具有优势,成本更低且结局更好;不确定性分析表明,从该卫生系统角度来看,鉴于支付意愿阈值为国际美元16,060(相当于果阿邦的人均国内生产总值)每获得一个质量调整生命年,HAP有95%的可能性具有成本效益。3个月时患者报告的行为激活水平介导了HAP干预对12个月抑郁得分的影响(β = -2.62;95%置信区间 -3.28,-1.97;p < 0.001)。严重不良事件很少见,两组患病率相似。我们无法评估随机分组后3个月和12个月结局评估时间点之间可能发生的缓解和复发情况。我们没有考虑或评估除行为激活之外的调节因子的影响。
治疗结束时HAP相对于EUC的优势在很大程度上随时间保持稳定,且由患者激活介导。从涵盖公共资助医疗服务以及对患者及其家庭生产力影响的角度来看,HAP以更低成本提供了更好的结局。
国际标准随机对照试验编号ISRCTN95149997