Plasencia Chamaida, Jurado Teresa, Villalba Alejandro, Peitedado Diana, Casla Maria Teresa López, Nuño Laura, Bonilla María Gema, Martínez-Feito Ana, Martín-Mola Emilio, Pascual-Salcedo Dora, Balsa Alejandro
Rheumatology Unit, Instituto de Investigación Sanitaria del Hospital Universitario La Paz (IdiPAZ) , Madrid , Spain.
Immunology Unit, Instituto de Investigación Sanitaria del Hospital Universitario La Paz (IdiPAZ) , Madrid , Spain.
Front Med (Lausanne). 2015 Oct 8;2:71. doi: 10.3389/fmed.2015.00071. eCollection 2015.
Evidence supporting treatment intensification in rheumatoid arthritis (RA) is limited and controversial. We explored outcomes of infliximab dose increases and accounted for pre-existing trough levels in patients with active RA.
This study was a retrospective study of 42 RA patients who received increased infliximab following an insufficient response (DAS28 >3.2). Serum concentrations of infliximab and antibodies to infliximab (ATI) and DAS28 and EULAR clinical response parameters were recorded for 1 year. Analyses were performed in three patient groups that were defined by infliximab serum concentration prior to treatment enhancement: no detectable, low (<1.1 μg/mL) or high (≥1.1 μg/mL) drug levels.
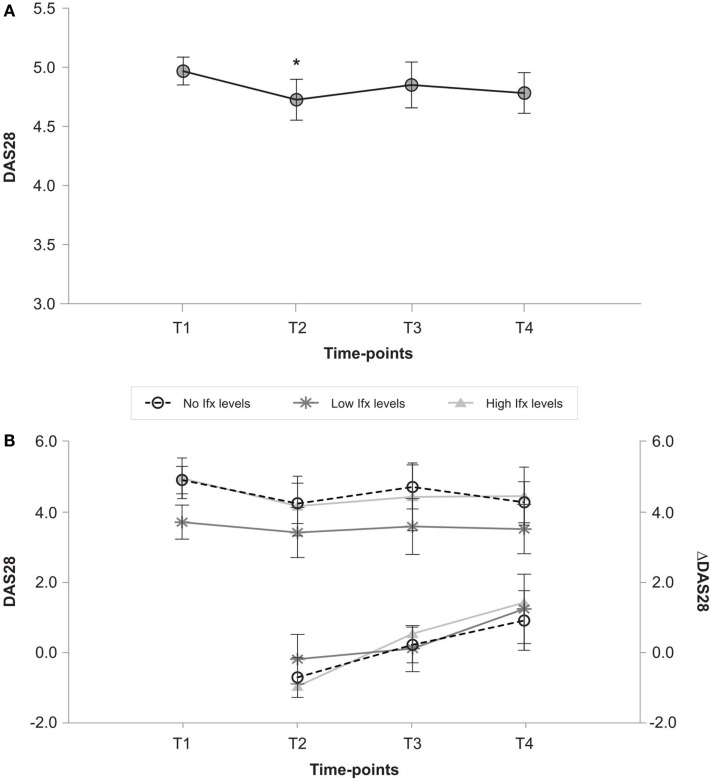
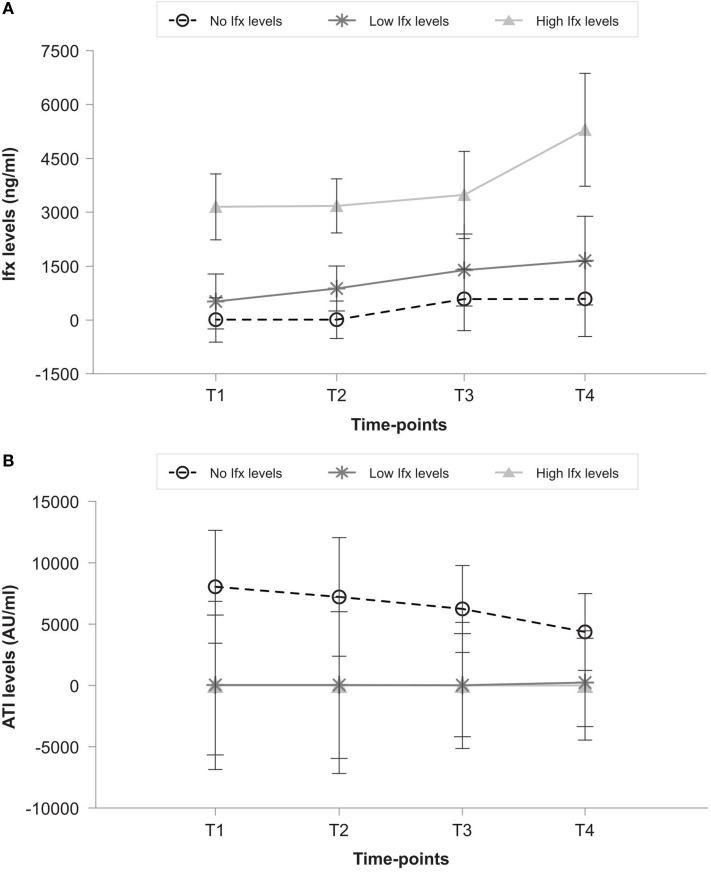
No circulating infliximab was detected in 20 patients (47.6%), but 13 (31%) and 9 (21.4%) patients exhibited low and high levels, respectively. ATI was only detected in patients with no detectable drug levels because the drug interferes with ELISA. DAS28 disease activity globally showed a modest improvement after dose escalation, but this improvement did not persist after 6 and 12 months. Infliximab serum levels increased significantly in the high group (p = 0.016), but no increase was achieved in the low and no detectable groups. The three study groups exhibited similar disease activity over time, and no improvement was observed in the non-responder EULAR rates.
These results suggest that the efficacy of an infliximab dose increase is limited, and the response is independent of the infliximab trough serum concentration that is achieved prior to escalation.
支持类风湿关节炎(RA)强化治疗的证据有限且存在争议。我们探讨了英夫利昔单抗剂量增加的疗效,并考虑了活动性RA患者预先存在的谷浓度。
本研究是一项回顾性研究,纳入42例对英夫利昔单抗反应不足(DAS28>3.2)后接受剂量增加治疗的RA患者。记录患者1年的英夫利昔单抗血清浓度、抗英夫利昔单抗抗体(ATI)、DAS28以及欧洲抗风湿病联盟(EULAR)临床反应参数。根据治疗强化前英夫利昔单抗血清浓度将患者分为三组进行分析:未检测到、低浓度(<1.1μg/mL)或高浓度(≥1.1μg/mL)。
20例患者(47.6%)未检测到循环中的英夫利昔单抗,但分别有13例(31%)和9例(21.4%)患者呈现低浓度和高浓度。仅在未检测到药物浓度的患者中检测到ATI,因为该药物会干扰酶联免疫吸附测定(ELISA)。剂量增加后,DAS28疾病活动度总体有适度改善,但在6个月和12个月后这种改善未持续。高浓度组英夫利昔单抗血清水平显著升高(p = 0.016),但低浓度组和未检测到组未升高。随着时间推移,三个研究组的疾病活动度相似,在无反应的EULAR率方面未观察到改善。
这些结果表明,增加英夫利昔单抗剂量的疗效有限,且反应与剂量增加前达到的英夫利昔单抗谷血清浓度无关。