Wang Weining, Iyer N Gopalakrishna, Tay Hsien Ts'ung, Wu Yonghui, Lim Tony K H, Zheng Lin, Song In Chin, Kwoh Chee Keong, Huynh Hung, Tan Patrick O B, Chow Pierce K H
Cellular and Molecular Research, National Cancer Centre, Singapore, 169610, Singapore.
Department of Surgical Oncology, National Cancer Centre Singapore, Singapore, 169610, Singapore.
BMC Cancer. 2015 Oct 31;15:828. doi: 10.1186/s12885-015-1814-8.
Despite advances in therapeutics, outcomes for hepatocellular carcinoma (HCC) remain poor and there is an urgent need for efficacious systemic therapy. Unfortunately, drugs that are successful in preclinical studies often fail in the clinical setting, and we hypothesize that this is due to functional differences between primary tumors and commonly used preclinical models. In this study, we attempt to answer this question by comparing tumor morphology and gene expression profiles between primary tumors, xenografts and HCC cell lines.
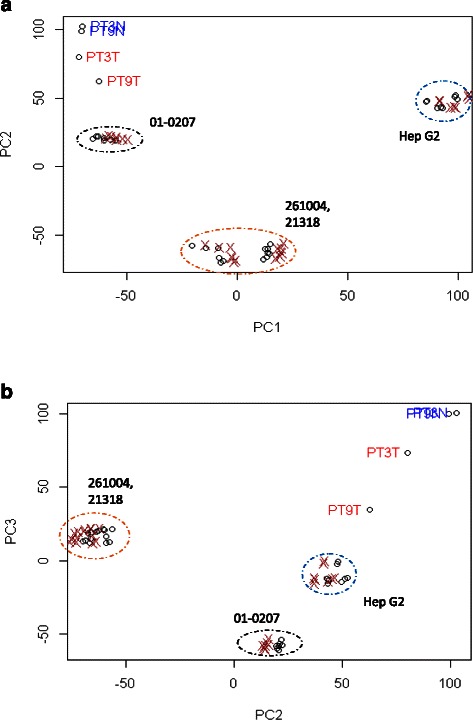
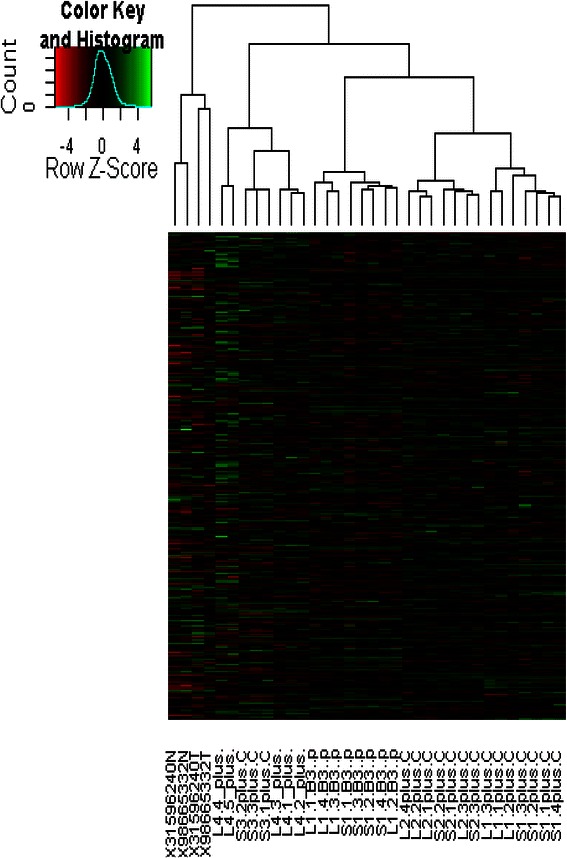
Hep G2 cell lines and tumor cells from patient tumor explants were subcutaneously (ectopically) injected into the flank and orthotopically into liver parenchyma of Mus Musculus SCID mice. The mice were euthanized after two weeks. RNA was extracted from the tumors, and gene expression profiling was performed using the Gene Chip Human Genome U133 Plus 2.0. Principal component analyses (PCA) and construction of dendrograms were conducted using Partek genomics suite.
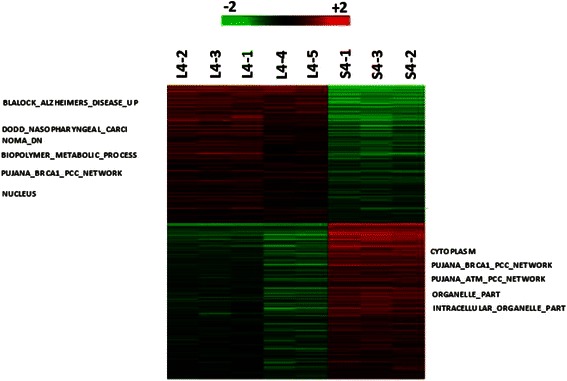
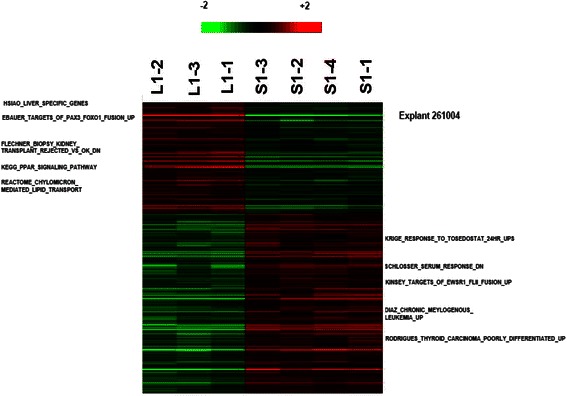
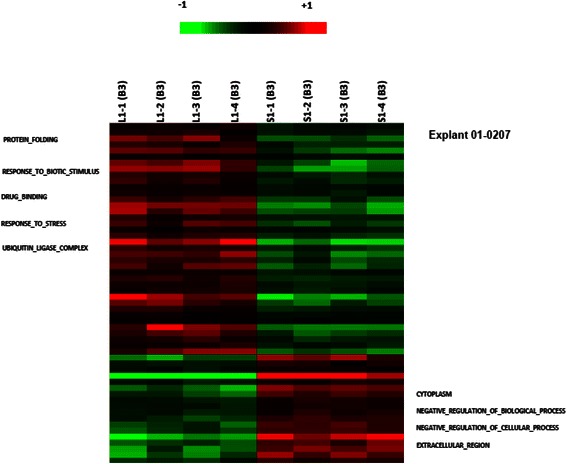
PCA showed that the commonly used HepG2 cell line model and its xenograft counterparts were vastly different from all fresh primary tumors. Expression profiles of primary tumors were also significantly divergent from their counterpart patient-derived xenograft (PDX) models, regardless of the site of implantation. Xenografts from the same primary tumors were more likely to cluster together regardless of site of implantation, although heat maps showed distinct differences in gene expression profiles between orthotopic and ectopic models.
The data presented here challenges the utility of routinely used preclinical models. Models using HepG2 were vastly different from primary tumors and PDXs, suggesting that this is not clinically representative. Surprisingly, site of implantation (orthotopic versus ectopic) resulted in limited impact on gene expression profiles, and in both scenarios xenografts differed significantly from the original primary tumors, challenging the long-held notion that orthotopic PDX model is the gold standard preclinical model for HCC.
尽管治疗方法有所进步,但肝细胞癌(HCC)的治疗效果仍然不佳,迫切需要有效的全身治疗。不幸的是,在临床前研究中成功的药物在临床环境中往往失败,我们推测这是由于原发性肿瘤与常用临床前模型之间的功能差异所致。在本研究中,我们试图通过比较原发性肿瘤、异种移植瘤和肝癌细胞系之间的肿瘤形态和基因表达谱来回答这个问题。
将Hep G2细胞系和患者肿瘤外植体的肿瘤细胞皮下(异位)注射到小鼠腹部,并原位注射到SCID小鼠的肝实质中。两周后对小鼠实施安乐死。从肿瘤中提取RNA,并使用基因芯片人类基因组U133 Plus 2.0进行基因表达谱分析。使用Partek基因组学套件进行主成分分析(PCA)和构建树状图。
PCA显示,常用的HepG2细胞系模型及其异种移植对应物与所有新鲜原发性肿瘤有很大不同。原发性肿瘤的表达谱也与其对应的患者来源异种移植(PDX)模型有显著差异,无论植入部位如何。来自同一原发性肿瘤的异种移植瘤更有可能聚集在一起,无论植入部位如何,尽管热图显示原位模型和异位模型之间的基因表达谱存在明显差异。
本文提供的数据对常规使用的临床前模型的实用性提出了挑战。使用HepG2的模型与原发性肿瘤和PDX有很大不同,表明其不具有临床代表性。令人惊讶的是,植入部位(原位与异位)对基因表达谱的影响有限,并且在两种情况下,异种移植瘤与原始原发性肿瘤都有显著差异,这对长期以来认为原位PDX模型是肝癌临床前模型的金标准这一观念提出了挑战。