Kasahara Yusuke, Izawa Kazuhiro P, Watanabe Satoshi, Osada Naohiko, Omiya Kazuto
Department of Rehabilitation Medicine, St. Marianna University School of Medicine, Yokohama City Seibu Hospital, Yokohama, Japan.
Graduate School of Health Sciences, Kobe University, Kobe, Japan.
Res Cardiovasc Med. 2015 Sep 15;4(4):e28944. doi: 10.5812/cardiovascmed.28944. eCollection 2015 Nov.
Breathlessness is a common problem in chronic heart failure (CHF) patients, and respiratory muscle strength has been proposed to play an important role in causing breathlessness in these patients.
The aim of this study was to investigate the relation between respiratory muscle strength and the severity of CHF, and the influence of respiratory muscle strength on abnormal ventilation during exercise in CHF patients.
In this case series study, we assessed clinically stable CHF outpatients (N = 66, age: 57.7 ± 14.6 years). The peak oxygen consumption (peak VO2), the slope relating minute ventilation to carbon dioxide production (VE/VCO2 slope), and the slope relating tidal volume to respiratory rate (TV/RR slope) were measured during cardiopulmonary exercise testing. Respiratory muscle strength was assessed by measuring the maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP).
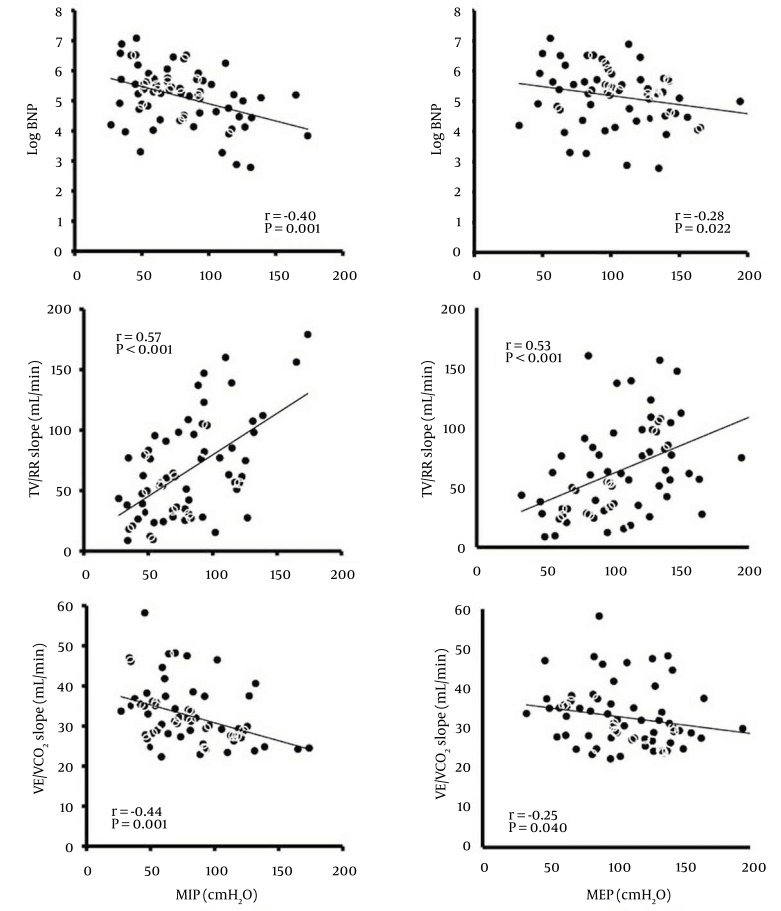
The MIP and MEP decreased significantly as the New York Heart Association functional class increased (MIP, P = 0.021; MEP, P < 0.01). The MIP correlated with the TV/RR slope (r = 0.57, P < 0.001) and the VE/VCO2 slope (r = -0.44, P < 0.001), and the MEP also correlated with the TV/RR slope (r = 0.53, P < 0.001) and the VE/VCO2 slope (r = -0.25, P < 0.040). Stepwise multiple regression analysis revealed that age and MIP were statistically significant predictors of the TV/RR and VE/VCO2 slopes (both P < 0.05).
Respiratory muscle strength is related to the severity of CHF, and associated with rapid and shallow ventilation or excessive ventilation during exercise.
呼吸困难是慢性心力衰竭(CHF)患者的常见问题,呼吸肌力量被认为在导致这些患者呼吸困难方面起重要作用。
本研究旨在探讨呼吸肌力量与CHF严重程度之间的关系,以及呼吸肌力量对CHF患者运动期间异常通气的影响。
在本病例系列研究中,我们评估了临床稳定的CHF门诊患者(N = 66,年龄:57.7±14.6岁)。在心肺运动试验期间测量峰值耗氧量(峰值VO2)、分钟通气量与二氧化碳产生量的关系斜率(VE/VCO2斜率)以及潮气量与呼吸频率的关系斜率(TV/RR斜率)。通过测量最大吸气压力(MIP)和最大呼气压力(MEP)评估呼吸肌力量。
随着纽约心脏协会功能分级增加,MIP和MEP显著降低(MIP,P = 0.021;MEP,P < 0.01)。MIP与TV/RR斜率(r = 0.57,P < 0.001)和VE/VCO2斜率(r = -0.44,P < 0.001)相关,MEP也与TV/RR斜率(r = 0.53,P < 0.001)和VE/VCO2斜率(r = -0.25,P < 0.040)相关。逐步多元回归分析显示,年龄和MIP是TV/RR和VE/VCO2斜率的统计学显著预测因素(均P < 0.05)。
呼吸肌力量与CHF严重程度相关,并与运动期间的快速浅呼吸或过度通气有关。