Zhang Lu-Ning, Gao Yuan-Hong, Lan Xiao-Wen, Tang Jie, Su Zhen, Ma Jun, Deng Wuguo, OuYang Pu-Yun, Xie Fang-Yun
Department of Radiation Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, Guangdong, China.
Department of Experimental Research, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, Guangdong, China.
Oncotarget. 2015 Dec 22;6(41):44019-29. doi: 10.18632/oncotarget.5806.
Patients with stage II nasopharyngeal carcinoma were reported to benefit from adding cisplatin-based concurrent chemotherapy to two-dimensional conventional radiotherapy. But this benefit becomes uncertain in the intensity-modulated radiotherapy (IMRT) era, owing to its significant advantage.
We enrolled 661 low risk (T1N1M0, T2N0-1M0 or T3N0M0, the 2010 UICC/AJCC staging system) patients who underwent IMRT with or without concurrent chemotherapy. Particularly, patients with IMRT alone or IMRT plus cisplatin-based concurrent chemotherapy were equally matched using propensity-score matching method. Overall survival (OS), distant metastasis-free survival (DMFS) and locoregional relapse-free survival (LRFS) were assessed with Kaplan-Meier method, log-rank test and Cox regression.
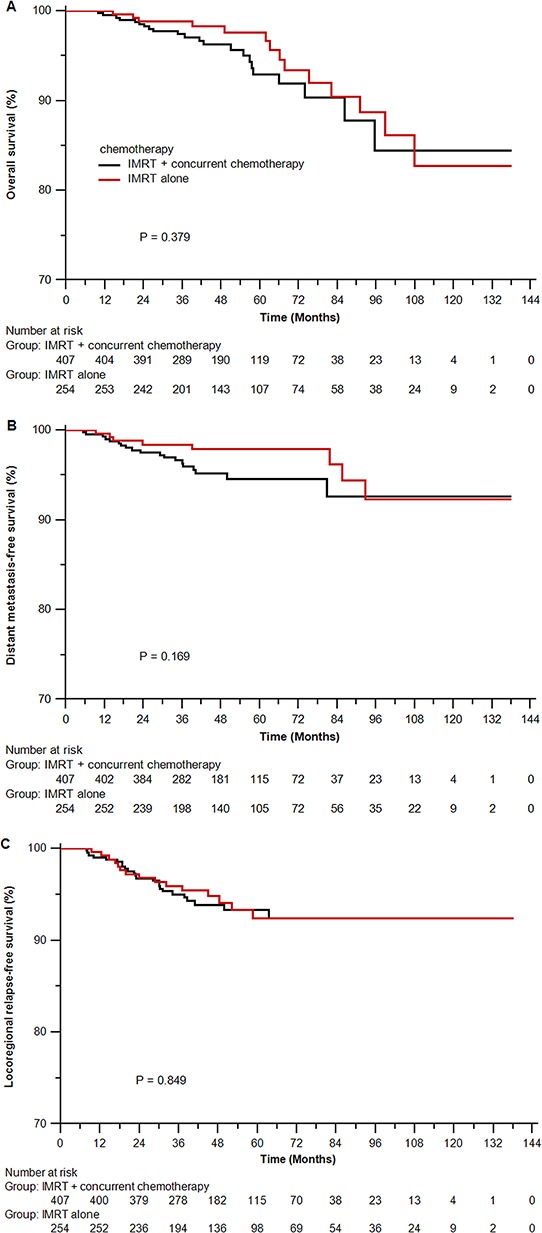
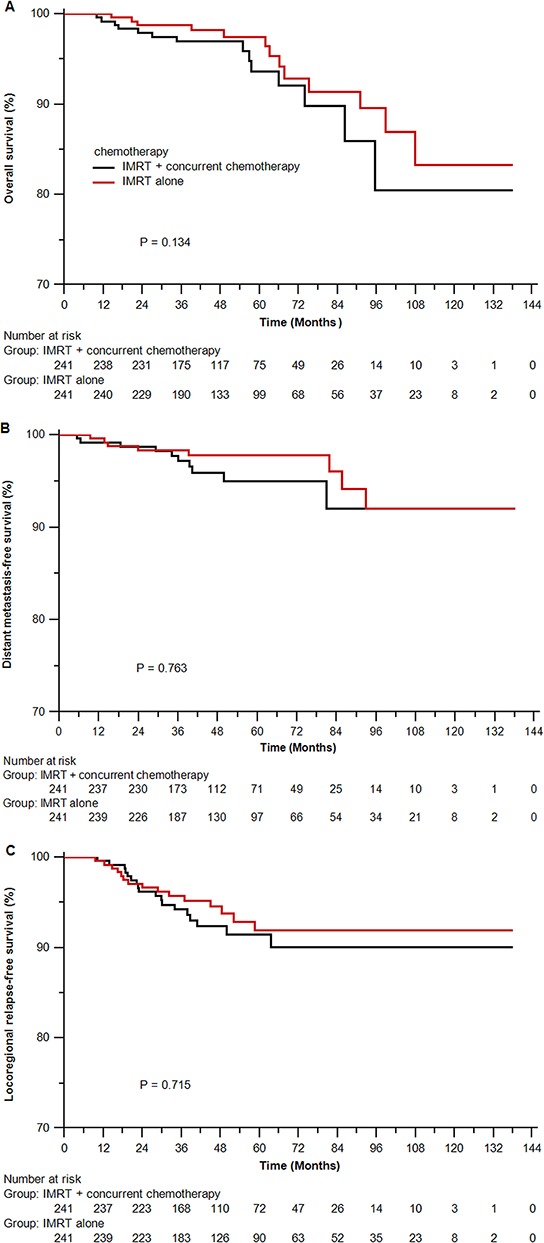
Among 661 patients, IMRT alone achieved parallel OS (P = 0.379), DMFS (P = 0.169) and LRFS (P = 0.849) to IMRT plus concurrent chemotherapy. In the propensity-matched cohort of 482 patients, similar survival were observed between both arms (4-years OS 97.4% vs 96.1%, P = 0.134; DMFS 96.5% vs 95.1%, P = 0.763; LRFS 93.8% vs 91.5%, P = 0.715). In multivariate analysis, cisplatin-based concurrent chemotherapy did not lower the risk of death, distant metastasis or locoregional relapse. And this association remained unchanged in subgroups by age, sex, histology and stage.
In this study, low risk nasopharyngeal carcinoma patients who underwent IMRT could not benefit from cisplatin-based concurrent chemotherapy.
据报道,II期鼻咽癌患者在二维传统放疗基础上加用顺铂同步化疗可获益。但在调强放疗(IMRT)时代,由于其显著优势,这种获益变得不确定。
我们纳入了661例低危(T1N1M0、T2N0 - 1M0或T3N0M0,2010年UICC/AJCC分期系统)患者,这些患者接受了IMRT联合或不联合同步化疗。具体而言,采用倾向评分匹配法使单纯IMRT或IMRT加顺铂同步化疗的患者达到均衡匹配。采用Kaplan - Meier法、对数秩检验和Cox回归评估总生存期(OS)、无远处转移生存期(DMFS)和无局部区域复发生存期(LRFS)。
在661例患者中,单纯IMRT的OS(P = 0.379)、DMFS(P = 0.169)和LRFS(P = 0.849)与IMRT加同步化疗相当。在482例倾向评分匹配队列中,两组的生存情况相似(4年OS 97.4%对96.1%,P = 0.134;DMFS 96.5%对95.1%,P = 0.763;LRFS 93.8%对91.5%,P = 0.715)。多因素分析显示,顺铂同步化疗并未降低死亡、远处转移或局部区域复发的风险。且在年龄、性别、组织学和分期亚组中,这种关联保持不变。
在本研究中,接受IMRT的低危鼻咽癌患者不能从顺铂同步化疗中获益。