Qiu Wen-Ze, Huang Pei-Yu, Shi Jun-Li, Xia Hai-Qun, Zhao Chong, Cao Ka-Jia
Department of Nasopharyngeal Carcinoma, State Key Laboratory of Oncology in South China, Collaborative Innovation Center of Cancer Medicine, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, 510060, P.R. China.
Department of Radiation Oncology, The Second Hospital of Tianjin Medical University, Tianjin, 300211, P.R. China.
Chin J Cancer. 2016 Jan 6;35:2. doi: 10.1186/s40880-015-0076-9.
In the era of intensity-modulated radiotherapy (IMRT), the role of neoadjuvant chemotherapy (NAC) for locoregionally advanced nasopharyngeal carcinoma (NPC) is under-evaluated. The aim of this study was to compare the efficacy of NAC plus IMRT and concurrent chemoradiotherapy (CCRT) plus adjuvant chemotherapy (AC) on locoregionally advanced NPC.
Between January 2004 and December 2008, 240 cases of locoregionally advanced NPC confirmed by pathologic assessment in Sun Yat-sen University Cancer Center were reviewed. Of the 240 patients, 117 received NAC followed by IMRT, and 123 were treated with CCRT plus AC. The NAC + IMRT group received a regimen that included cisplatin and 5-fluorouracil (5-FU). The CCRT + AC group received cisplatin concurrently with radiotherapy, and subsequently received adjuvant cisplatin and 5-FU. The survival rates were assessed by Kaplan-Meier analysis, and the survival curves were compared using a log-rank test. Multivariate analysis was conducted using the Cox proportional hazard regression model.
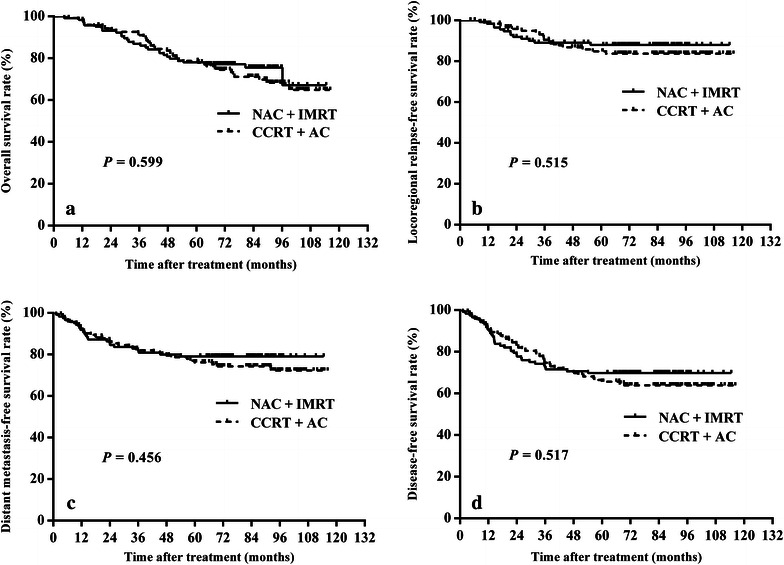
The 5-year overall survival (OS), locoregional relapse-free survival (LRRFS), distant metastasis-free survival (DMFS), and disease-free survival (DFS) were 78.0, 87.9, 79.0, and 69.8%, respectively, for the NAC + IMRT group and 78.7, 84.8, 76.2, and 65.6%, respectively, for the CCRT + AC group. There were no significant differences in survival between the two groups. In multivariate analysis, age (<50 years vs. ≥50 years) and overall stage (III vs. IV) were found to be independent predictors for OS and DFS; furthermore, the overall stage was a significant prognostic factor for DMFS. Compared with the CCRT + AC protocol, the NAC + IMRT protocol significantly reduced the occurrence rates of grade 3-4 nausea-vomiting (6.5 vs. 1.5%, P = 0.023) and leukopenia (9.7 vs. 0.8%, P = 0.006).
The treatment outcomes of the NAC + IMRT and CCRT + AC groups were similar. Distant metastasis remained the predominant mode of treatment failure.
在调强放射治疗(IMRT)时代,新辅助化疗(NAC)在局部晚期鼻咽癌(NPC)中的作用尚未得到充分评估。本研究旨在比较NAC联合IMRT与同步放化疗(CCRT)联合辅助化疗(AC)治疗局部晚期NPC的疗效。
回顾性分析2004年1月至2008年12月在中山大学肿瘤防治中心经病理评估确诊的240例局部晚期NPC患者。240例患者中,117例接受NAC后行IMRT,123例接受CCRT联合AC治疗。NAC + IMRT组接受包括顺铂和5-氟尿嘧啶(5-FU)的方案。CCRT + AC组在放疗时同步接受顺铂治疗,随后接受辅助顺铂和5-FU治疗。采用Kaplan-Meier分析评估生存率,使用对数秩检验比较生存曲线。采用Cox比例风险回归模型进行多因素分析。
NAC + IMRT组的5年总生存率(OS)、局部区域无复发生存率(LRRFS)、远处转移无复发生存率(DMFS)和无病生存率(DFS)分别为78.0%、87.9%、79.0%和69.8%,CCRT + AC组分别为78.7%、84.8%、76.2%和65.6%。两组生存率无显著差异。多因素分析发现,年龄(<50岁与≥50岁)和总体分期(III期与IV期)是OS和DFS的独立预测因素;此外,总体分期是DMFS的重要预后因素。与CCRT + AC方案相比,NAC + IMRT方案显著降低了3-4级恶心呕吐(6.5%对1.5%,P = 0.023)和白细胞减少(9.7%对0.8%,P = 0.006)的发生率。
NAC + IMRT组和CCRT + AC组的治疗效果相似。远处转移仍然是主要的治疗失败模式。