Di Filippo F, Giannarelli D, Bouteille C, Bernet L, Cano R, Cunnick G, Sapino A
Regina Elena National Cancer Institute, Via Elio Chianesi 53, 00134, Rome, Italy.
Clinique Mutualiste, Saint Etienne, France.
J Exp Clin Cancer Res. 2015 Nov 4;34:136. doi: 10.1186/s13046-015-0246-2.
Tumor-positive sentinel node(SLN) biopsy results in a risk of nonsentinel node metastases in case of micro and macro metastases ranging from 20 to 50 %, respectively. Therefore, most patients underwent unnecessary axillary lymph node dissections. Thus, the development of a mathematical model for predicting patient-specific risk of non sentinel node(NSLN) metastases is strongly warranted.
The following parameters were recorded:
hospital, age, medical record number Bio-pathological: tumor (T) size, grading (G), multifocality, histological type, LVI, ER-PR status, HER-2, ki67, molecular classification (luminal A, luminal B, HER2 like, triple negative) Sentinel and nonsentinel lymph node related: number of removed SLNs, number of positive and negative SLNs, copy number of positive sentinel nodes, ratio: number of positive SLNs to number of removed SLNs, number of removed and number of positive nodes after ALND. A total of 2460 patients have been included in the database. All the patients have been provided by the authors of this paper.
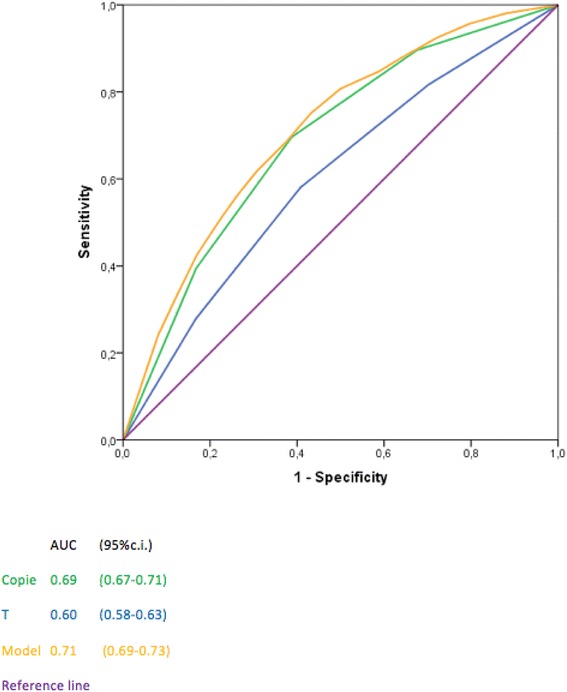
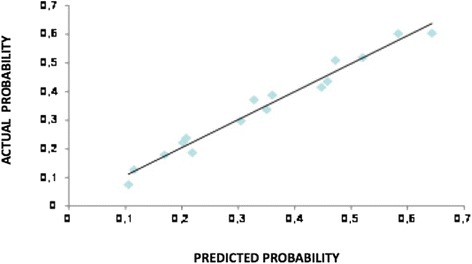
Multivariate logistic regression analysis demonstrated that only the number of a CK19 mRNA copies (p < 0.0001), T size (p < 0.0001) and LVI (p < 0.0001) were associated with NSN metastases. The discrimination of the model, quantified with the area under the receiver operating characteristics curve, was 0.71 (95 %, C.I. 0.69-0.73), thus confirming a good level of reliability.
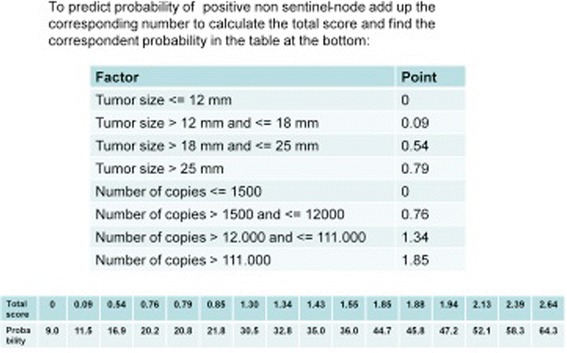
The nomogram may be employed by the surgeon as a decision making tool on whether to perform an intraoperative axillary lymph node dissection on breast cancer patients with SLN positive. The large population employed and the standardized method of measuring the value of CK19 mRNA copies are appropiate prerequisites for a reliable nomogram.
肿瘤阳性前哨淋巴结(SLN)活检结果显示,若存在微转移和宏转移,非前哨淋巴结转移风险分别为20%至50%。因此,大多数患者接受了不必要的腋窝淋巴结清扫术。因此,强烈需要开发一种数学模型来预测患者特异性的非前哨淋巴结(NSLN)转移风险。
记录了以下参数:
医院、年龄、病历号
肿瘤(T)大小、分级(G)、多灶性、组织学类型、淋巴管浸润(LVI)、雌激素受体-孕激素受体(ER-PR)状态、人表皮生长因子受体2(HER-2)、Ki67、分子分类(腔面A型、腔面B型、HER2过表达型、三阴性)
切除的前哨淋巴结数量、阳性和阴性前哨淋巴结数量、阳性前哨淋巴结的拷贝数、比率:阳性前哨淋巴结数量与切除的前哨淋巴结数量之比、腋窝淋巴结清扫术后切除的淋巴结数量和阳性淋巴结数量。数据库共纳入2460例患者。所有患者均由本文作者提供。
多因素逻辑回归分析表明,只有细胞角蛋白19(CK19)mRNA拷贝数(p<0.0001)、T大小(p<0.0001)和LVI(p<0.0001)与NSN转移相关。用受试者工作特征曲线下面积量化的模型鉴别力为0.71(95%置信区间0.69-0.73),从而证实了较高的可靠性水平。
该列线图可被外科医生用作决策工具,以决定是否对前哨淋巴结阳性的乳腺癌患者进行术中腋窝淋巴结清扫。纳入的大量人群以及测量CK19 mRNA拷贝数的标准化方法是可靠列线图的合适前提条件。