Dominguez Ligia J, Bes-Rastrollo Maira, Basterra-Gortari Francisco Javier, Gea Alfredo, Barbagallo Mario, Martínez-González Miguel A
Geriatric Unit, Department of Internal Medicine and Geriatrics, University of Palermo, Palermo, Italy.
Department of Preventive Medicine and Public Health, University of Navarra-IDISNA, Pamplona, Spain and CIBER Fisiopatologia de la Obesidad y Nutricion (CIBERobn), Instituto de Salud Carlos III, Madrid, Spain.
PLoS One. 2015 Nov 6;10(11):e0141760. doi: 10.1371/journal.pone.0141760. eCollection 2015.
Strong evidence supports that dietary modifications may decrease incident type 2 diabetes mellitus (T2DM). Numerous diabetes risk models/scores have been developed, but most do not rely specifically on dietary variables or do not fully capture the overall dietary pattern. We prospectively assessed the association of a dietary-based diabetes-risk score (DDS), which integrates optimal food patterns, with the risk of developing T2DM in the SUN ("Seguimiento Universidad de Navarra") longitudinal study.
We assessed 17,292 participants initially free of diabetes, followed-up for a mean of 9.2 years. A validated 136-item FFQ was administered at baseline. Taking into account previous literature, the DDS positively weighted vegetables, fruit, whole cereals, nuts, coffee, low-fat dairy, fiber, PUFA, and alcohol in moderate amounts; while it negatively weighted red meat, processed meats and sugar-sweetened beverages. Energy-adjusted quintiles of each item (with exception of moderate alcohol consumption that received either 0 or 5 points) were used to build the DDS (maximum: 60 points). Incident T2DM was confirmed through additional detailed questionnaires and review of medical records of participants. We used Cox proportional hazards models adjusted for socio-demographic and anthropometric parameters, health-related habits, and clinical variables to estimate hazard ratios (HR) of T2DM.
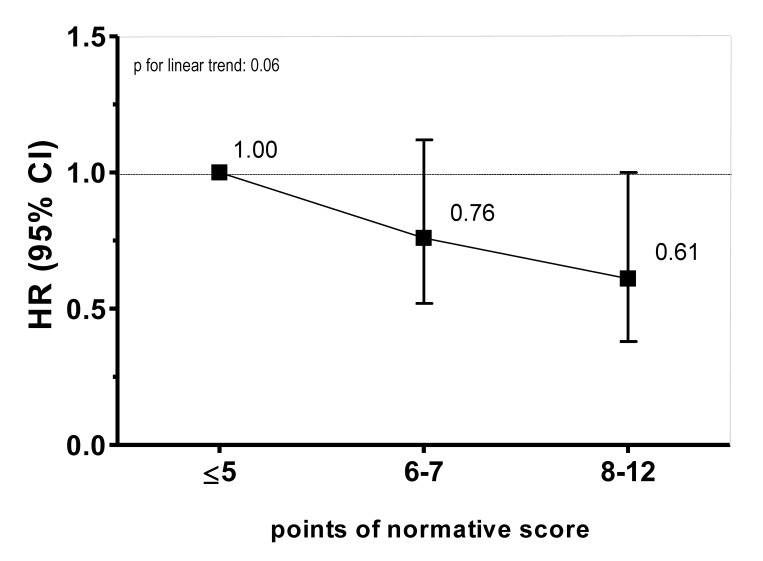
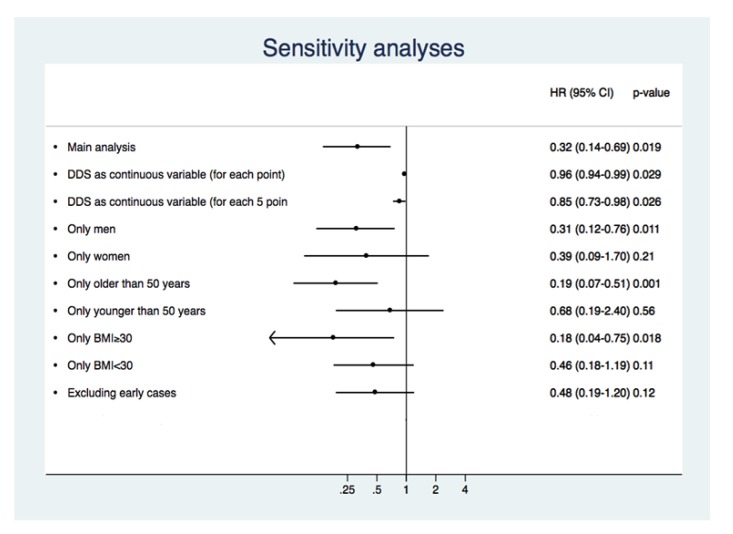
We observed 143 T2DM confirmed cases during follow-up. Better baseline conformity with the DDS was associated with lower incidence of T2DM (multivariable-adjusted HR for intermediate (25-39 points) vs. low (11-24) category 0.43 [95% confidence interval (CI) 0.21, 0.89]; and for high (40-60) vs. low category 0.32 [95% CI: 0.14, 0.69]; p for linear trend: 0.019).
The DDS, a simple score exclusively based on dietary components, showed a strong inverse association with incident T2DM. This score may be applicable in clinical practice to improve dietary habits of subjects at high risk of T2DM and also as an educational tool for laypeople to help them in self-assessing their future risk for developing diabetes.
有力证据支持饮食调整可能降低2型糖尿病(T2DM)的发病风险。已经开发了许多糖尿病风险模型/评分,但大多数并非专门依赖饮食变量,或者没有充分体现整体饮食模式。在“纳瓦拉大学随访研究”(SUN)纵向研究中,我们前瞻性评估了一种基于饮食的糖尿病风险评分(DDS)与T2DM发病风险的关联,该评分整合了最佳食物模式。
我们评估了17292名最初无糖尿病的参与者,平均随访9.2年。在基线时采用经过验证的136项食物频率问卷(FFQ)。考虑到既往文献,DDS对蔬菜、水果、全谷物、坚果、咖啡、低脂乳制品、纤维、多不饱和脂肪酸(PUFA)和适量饮酒给予正向加权;而对红肉、加工肉类和含糖饮料给予负向加权。每项的能量调整五分位数(适量饮酒除外,给予0或5分)用于构建DDS(最高分60分)。通过额外的详细问卷和参与者病历审查确认T2DM发病情况。我们使用经社会人口统计学和人体测量学参数、健康相关习惯及临床变量调整的Cox比例风险模型来估计T2DM的风险比(HR)。
随访期间我们观察到143例确诊的T2DM病例。基线时与DDS的符合程度越高,T2DM发病率越低(中间五分位数(25 - 39分)与低五分位数(11 - 24分)相比,多变量调整后的HR为0.43 [95%置信区间(CI)0.21, 0.89];高五分位数(40 - 60分)与低五分位数相比,HR为0.32 [95% CI:0.14, 0.69];线性趋势p值:0.019)。
DDS是一个仅基于饮食成分的简单评分,与T2DM发病呈强烈负相关。该评分可应用于临床实践,以改善T2DM高危人群的饮食习惯,也可作为一种教育工具,帮助外行人自我评估其未来患糖尿病的风险。