Lagarde S M, Phillips A W, Navidi M, Disep B, Immanuel A, Griffin S M
Northern Oesophago-Gastric Cancer Unit, Royal Victoria Infirmary, Queen Victoria Road, Newcastle-Upon-Tyne NE1 4LP, UK.
Br J Cancer. 2015 Nov 17;113(10):1427-33. doi: 10.1038/bjc.2015.354. Epub 2015 Nov 10.
In patients treated for oesophageal cancer the importance of lymphovascular and perineural invasion (PNI) after neoadjuvant therapy has yet to be established. The aim of this study was to assess the incidence and prognostic significance of these factors in a consecutive series of patients with cancer of the oesophagus or gastro-oesophageal junction (GOJ) who underwent neoadjuvant therapy followed by oesophagectomy.
Clinical and pathology results from patients with potentially curable adenocarcinoma, or squamous cell carcinoma of the oesophagus or GOJ were reviewed. Patients were treated with neoadjuvant chemotherapy or chemoradiation followed by transthoracic oesophagectomy and two-field lymphadenectomy. The presence of venous invasion (VI), lymph vessel invasion (LI) and perineural invasion (PNI) were correlated with clinical outcomes.
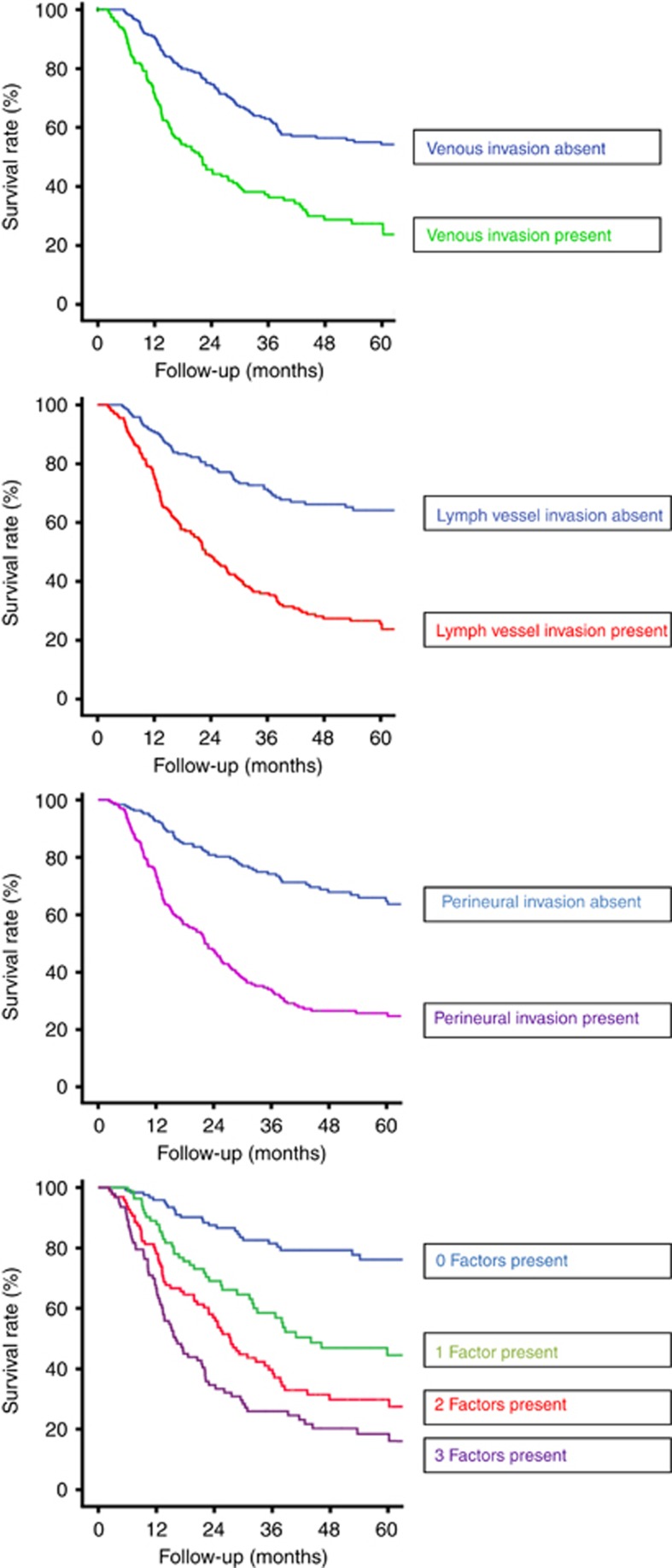
A total of 396 patients underwent oesophagectomy after neoadjuvant therapy for oesophageal cancer. Venous invasion was identified in 150 (38%) of patients, LI in 203 (51%) patients and PNI in 204 (52%) patients. In all, 123 (31%) patients had no evidence of either VI, LI or PNI. A total of 96 (24%) had a combination of two factors and 94 (24%) had all three factors. The presence of VI, LI and PNI was significantly related to tumour stage (P=0.001). Median overall survival was 170.8 months when all three factors were absent, 44.0 months when one factor was present, 27.1 months when two factors were present and 16.0 months when all were present. Multivariate analyses revealed VI, LI and PNI or a combination of these factors were independent predictors of prognosis.
In oesophageal cancer patients treated with neoadjuvant therapy followed by oesophagectomy the presence of VI, LI and PNI has an important prognostic impact and may identify patients at high risk of recurrence who would benefit from adjuvant therapies.
在接受食管癌治疗的患者中,新辅助治疗后血管淋巴管浸润和神经周围浸润(PNI)的重要性尚未明确。本研究的目的是评估这些因素在一系列连续接受新辅助治疗后行食管切除术的食管癌或胃食管交界(GOJ)癌患者中的发生率及预后意义。
回顾了潜在可治愈的食管腺癌、鳞状细胞癌或GOJ癌患者的临床和病理结果。患者接受新辅助化疗或放化疗,随后行开胸食管切除术和二野淋巴结清扫术。静脉浸润(VI)、淋巴管浸润(LI)和神经周围浸润(PNI)的存在与临床结局相关。
共有396例患者在新辅助治疗食管癌后接受了食管切除术。150例(38%)患者存在静脉浸润,203例(51%)患者存在淋巴管浸润,204例(52%)患者存在神经周围浸润。共有123例(31%)患者未发现VI、LI或PNI。共有96例(24%)患者存在两种因素,94例(24%)患者存在所有三种因素。VI、LI和PNI的存在与肿瘤分期显著相关(P=0.001)。当三种因素均不存在时,中位总生存期为170.8个月;当存在一种因素时,为44.0个月;当存在两种因素时,为27.1个月;当三种因素均存在时,为16.0个月。多变量分析显示,VI、LI和PNI或这些因素的组合是预后的独立预测因素。
在接受新辅助治疗后行食管切除术的食管癌患者中,VI、LI和PNI的存在具有重要的预后影响,可能识别出复发风险高且将从辅助治疗中获益的患者。