Hippisley-Cox Julia, Coupland Carol
Division of Primary Care, Nottingham University, Nottingham NG2 7RD, UK
Division of Primary Care, Nottingham University, Nottingham NG2 7RD, UK.
BMJ. 2015 Nov 11;351:h5441. doi: 10.1136/bmj.h5441.
Is it possible to develop and externally validate risk prediction equations to estimate the 10 year risk of blindness and lower limb amputation in patients with diabetes aged 25-84 years?
This was a prospective cohort study using routinely collected data from general practices in England contributing to the QResearch and Clinical Practice Research Datalink (CPRD) databases during the study period 1998-2014. The equations were developed using 763 QResearch practices (n=454,575 patients with diabetes) and validated in 254 different QResearch practices (n=142,419) and 357 CPRD practices (n=206,050). Cox proportional hazards models were used to derive separate risk equations for blindness and amputation in men and women that could be evaluated at 10 years. Measures of calibration and discrimination were calculated in the two validation cohorts.
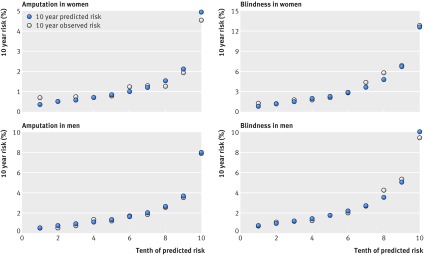
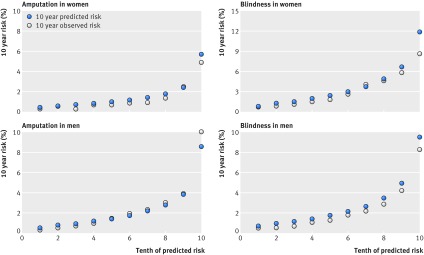
Risk prediction equations to quantify absolute risk of blindness and amputation in men and women with diabetes have been developed and externally validated. In the QResearch derivation cohort, 4822 new cases of lower limb amputation and 8063 new cases of blindness occurred during follow-up. The risk equations were well calibrated in both validation cohorts. Discrimination was good in men in the external CPRD cohort for amputation (D statistic 1.69, Harrell's C statistic 0.77) and blindness (D statistic 1.40, Harrell's C statistic 0.73), with similar results in women and in the QResearch validation cohort. The algorithms are based on variables that patients are likely to know or that are routinely recorded in general practice computer systems. They can be used to identify patients at high risk for prevention or further assessment. Limitations include lack of formally adjudicated outcomes, information bias, and missing data.
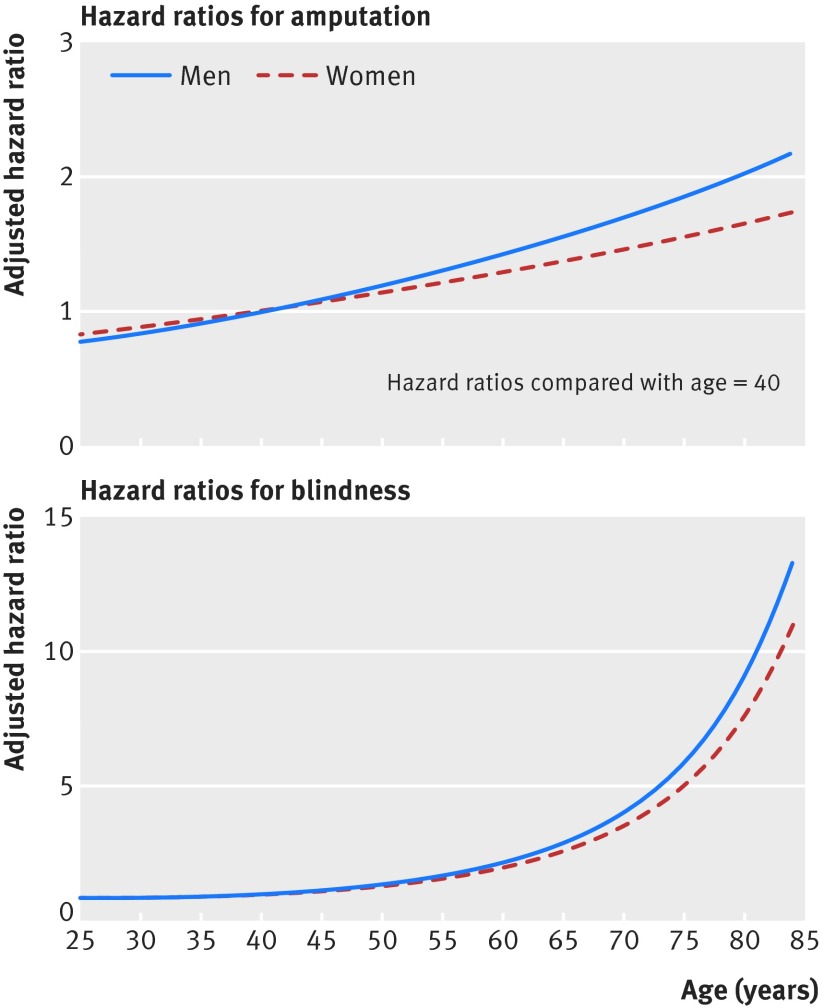
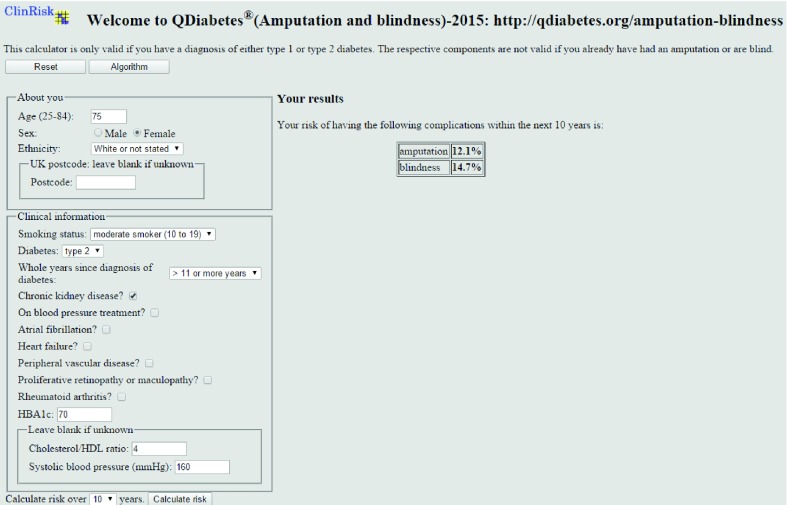
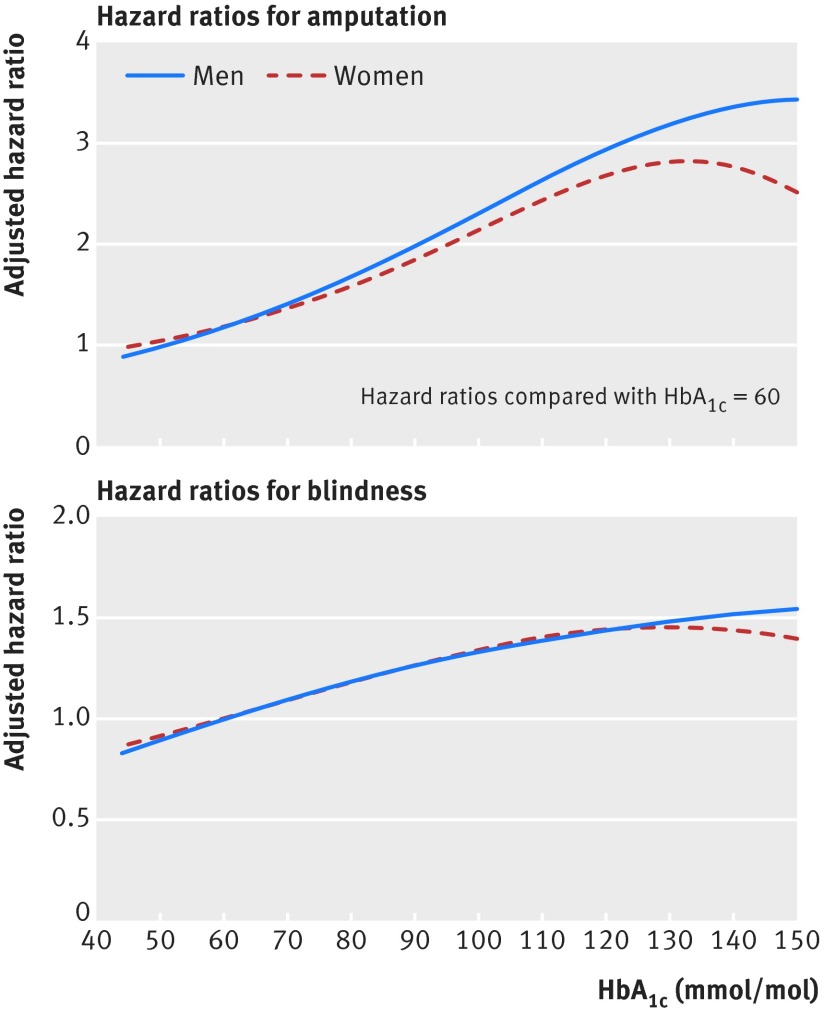
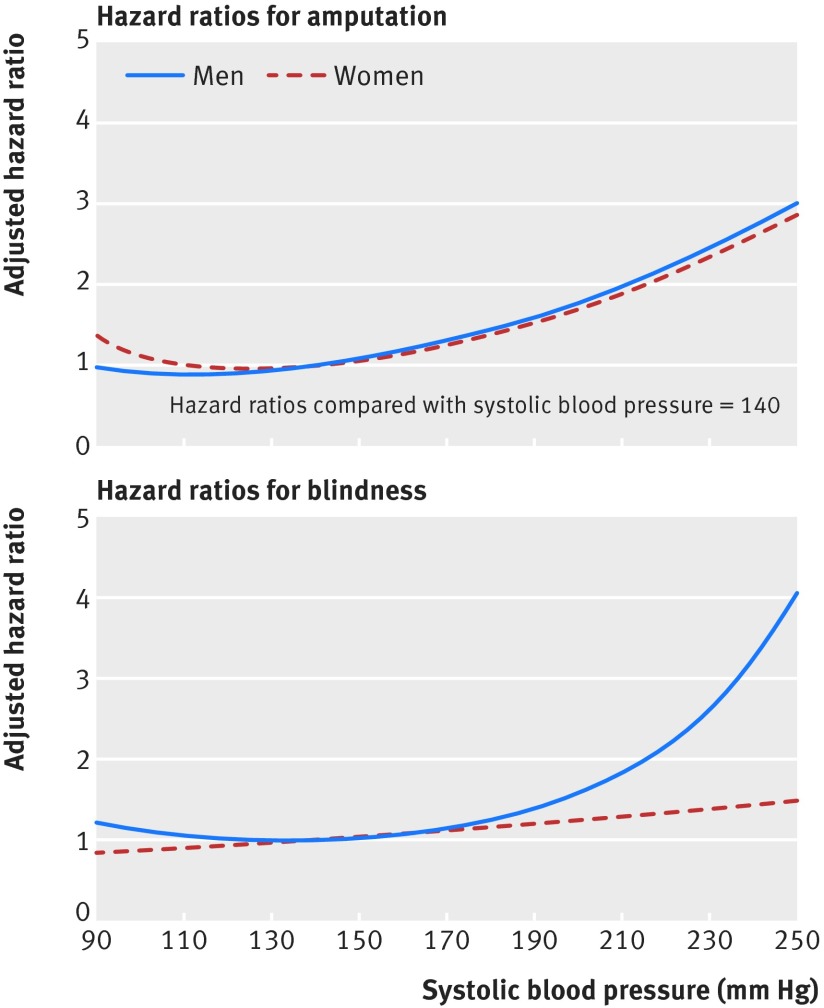
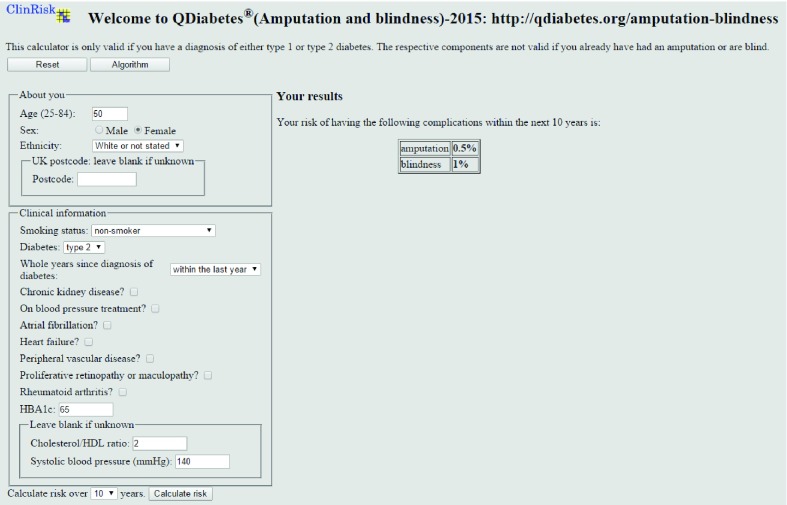
Patients with type 1 or type 2 diabetes are at increased risk of blindness and amputation but generally do not have accurate assessments of the magnitude of their individual risks. The new algorithms calculate the absolute risk of developing these complications over a 10 year period in patients with diabetes, taking account of their individual risk factors.
FUNDING, COMPETING INTERESTS, DATA SHARING: JH-C is co-director of QResearch, a not for profit organisation which is a joint partnership between the University of Nottingham and Egton Medical Information Systems, and is also a paid director of ClinRisk Ltd. CC is a paid consultant statistician for ClinRisk Ltd.
是否有可能开发并外部验证风险预测方程,以估计25至84岁糖尿病患者10年内失明和下肢截肢的风险?
这是一项前瞻性队列研究,使用了在1998年至2014年研究期间从英格兰普通诊所常规收集的数据,这些数据被纳入QResearch和临床实践研究数据链(CPRD)数据库。该方程是利用763个QResearch诊所(454575例糖尿病患者)的数据开发的,并在254个不同的QResearch诊所(142419例患者)和357个CPRD诊所(206050例患者)中进行了验证。使用Cox比例风险模型分别推导男性和女性失明和截肢的风险方程,并在10年内进行评估。在两个验证队列中计算了校准和区分度的指标。
已开发并外部验证了用于量化糖尿病男性和女性失明和截肢绝对风险的风险预测方程。在QResearch推导队列中,随访期间发生了4822例下肢截肢新病例和8063例失明新病例。风险方程在两个验证队列中校准良好。在外部CPRD队列中,男性截肢(D统计量1.69,Harrell's C统计量0.77)和失明(D统计量1.40,Harrell's C统计量0.73)的区分度良好,女性和QResearch验证队列的结果相似。这些算法基于患者可能知晓或在普通诊所计算机系统中常规记录的变量。它们可用于识别高危患者以进行预防或进一步评估。局限性包括缺乏正式判定的结果、信息偏倚和数据缺失。
1型或2型糖尿病患者失明和截肢的风险增加,但通常对其个体风险的严重程度没有准确评估。新算法考虑了糖尿病患者的个体风险因素,计算了他们在10年内发生这些并发症的绝对风险。
资金、竞争利益、数据共享:JH - C是QResearch的联合主任,QResearch是一家非营利组织,是诺丁汉大学和埃格顿医学信息系统的联合合作伙伴,JH - C也是ClinRisk Ltd的付费董事。CC是ClinRisk Ltd的付费顾问统计学家。