McHugh Kimberly E, Pasquali Sara K, Hall Matthew A, Scheurer Mark A
1Medical University of South Carolina,Charleston,South Carolina,United States of America.
2University of Michigan CS Mott Children's Hospital,Ann Arbor,Michigan,United States of America.
Cardiol Young. 2016 Oct;26(7):1303-9. doi: 10.1017/S1047951115002498. Epub 2015 Dec 30.
Introduction Patients undergoing the Norwood operation consume considerable healthcare resources; however, detailed information regarding factors impacting hospitalisation costs is lacking. We evaluated the association of postoperative complications with hospital costs.
In the present study, we utilised a unique data set consisting of prospectively collected clinical data from the Pediatric Heart Network Single Ventricle Reconstruction trial linked at the patient level with cost data for 10 hospitals participating in the Children's Hospital Association Case Mix database during the trial period. The relationship between complications and cost was modelled using linear regression, accounting for the skewed distribution of cost, adjusting for within-centre clustering and baseline patient characteristics.
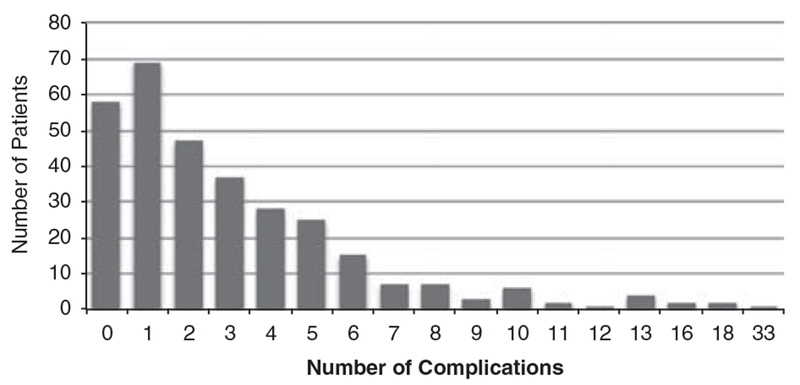
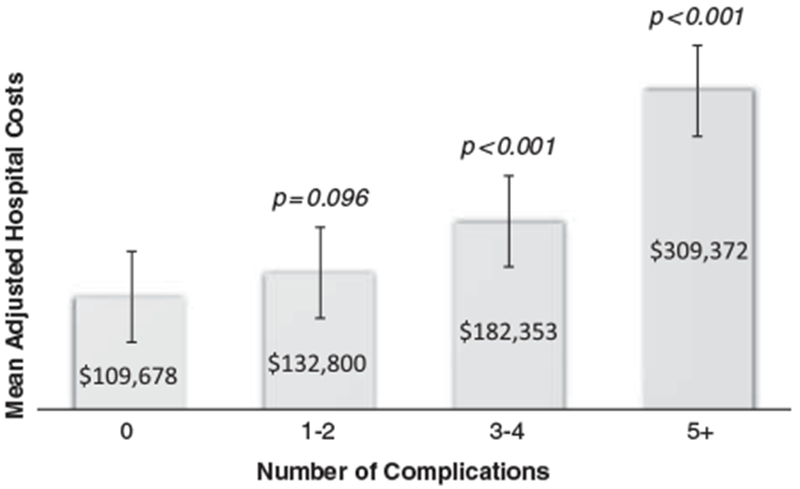
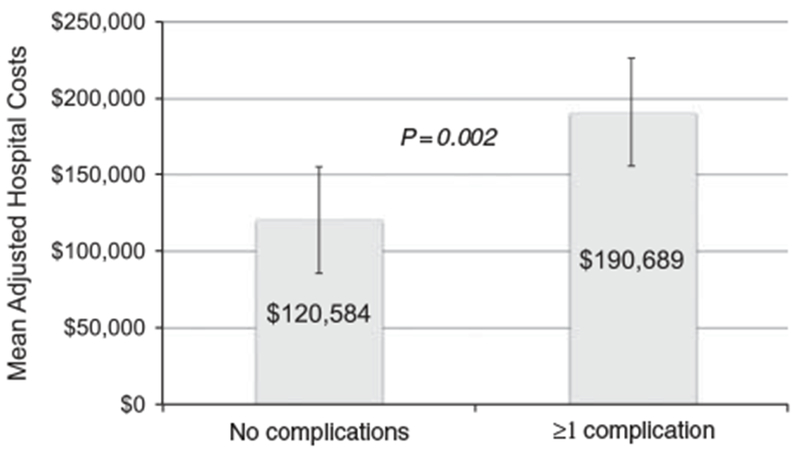
A total of 334 eligible Norwood records (97.5%) were matched between data sets. Overall, 82% suffered from at least one complication (median 2; with a range from 0 to 33). Those with complications had longer postoperative length of stay (25 versus 12 days, p<0.001), more total ventilator days (7 versus 5 days, p<0.001), and higher in-hospital mortality (17.6 versus 3.4%, p<0.006). Mean adjusted hospital cost in those with a complication was $190,689 (95% CI $111,344-$326,577) versus $120,584 (95% CI $69,246-$209,983) in those without complications (p=0.002). Costs increased with the number of complications (1-2 complications=$132,800 versus 3-4 complications=$182,353 versus ⩾5 complications=$309,372 [p<0.001]).
This merged data set of clinical trial and cost data demonstrated that postoperative complications are common following the Norwood operation and are associated with worse clinical outcomes and higher costs. Efforts to reduce complications in this population may lead to improved outcomes and cost savings.
引言 接受诺伍德手术的患者消耗了大量医疗资源;然而,关于影响住院费用因素的详细信息却很缺乏。我们评估了术后并发症与住院费用之间的关联。
在本研究中,我们使用了一个独特的数据集,该数据集由前瞻性收集的来自儿科心脏网络单心室重建试验的临床数据组成,在患者层面与试验期间参与儿童医院协会病例组合数据库的10家医院的费用数据相链接。并发症与费用之间的关系采用线性回归模型进行建模,考虑到费用的偏态分布,对中心内聚类和基线患者特征进行了调整。
共有334条符合条件的诺伍德记录(97.5%)在数据集之间匹配成功。总体而言,82%的患者至少出现一种并发症(中位数为2;范围为0至33)。出现并发症的患者术后住院时间更长(25天对12天,p<0.001),总机械通气天数更多(7天对5天,p<0.001),院内死亡率更高(17.6%对3.4%,p<0.006)。出现并发症患者的平均调整后住院费用为190,689美元(95%置信区间为111,344美元至326,577美元),而未出现并发症患者的平均调整后住院费用为120,584美元(95%置信区间为69,246美元至209,983美元)(p=0.002)。费用随着并发症数量的增加而增加(1至2种并发症为132,800美元,3至4种并发症为182,353美元,≥5种并发症为309,372美元 [p<0.001])。
这个临床试验和费用数据的合并数据集表明,诺伍德手术后术后并发症很常见,并且与更差的临床结果和更高的费用相关。减少该人群并发症的努力可能会改善结果并节省费用。