Mugwagwa Norma, Mberikunashe Joseph, Gombe Notion Tafara, Tshimanga Mufuta, Bangure Donewell, Mungati More
Department of Community Medicine, University of Zimbabwe, Office 3-66 Kaguvi Building, Corner 4th/Central Avenue, Harare, Zimbabwe.
Ministry of Health and Child Care, Harare, Zimbabwe.
BMC Res Notes. 2015 Dec 29;8:829. doi: 10.1186/s13104-015-1831-3.
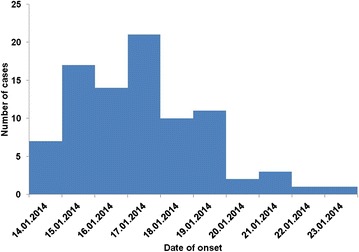
In January of 2014, an outbreak of malaria was declared in the Honde Valley region of Mutasa District in Zimbabwe. The area has a hot, temperate climate and high rainfall pattern ideal for vector breeding and malaria transmission. Gravity fed irrigation channels span the valley creating a number of breeding sites for malaria vectors, mosquitoes. Malaria outbreaks have been a common occurrence in the district over the past few years despite the district meeting set targets for prevention interventions like indoor residual spraying (IRS) with pyrethroids and long lasting insecticidal nets distribution. The objectives of this study were to describe the outbreak by person, place and time, to assess the community's knowledge on malaria transmission, signs and symptoms and treatment and to tease out factors associated with malaria infection in the district.
An unmatched case-control study was carried out. Interviewer guided questionnaires were administered to residents of the valley who met the inclusion criteria in order to tease out possible factors associated with malaria infection. A case was defined as a resident of Honde Valley with a history of malaria symptoms and a confirmed diagnosis from 13 January 2014 to 26 January 2014. A control was a resident of Mutasa District who was present in the district during the time of the outbreak but did not develop symptoms of malaria. A total of 87 cases and 87 controls were enrolled.
Cases and controls were comparable in terms of socio-demographic characteristics and knowledge on malaria transmission, treatment and prevention. Risk factors associated with contracting malaria during the outbreak were being under the age of 5 years (OR = 9.92, CI 1, 2-80, 1), not using mosquito repellents (OR = 8, 25 CI 3, 78-18, 0), having outdoor activities before dawn and after dusk (OR = 2, 81 CI 1,04-7, 6). Having received indoor residual spraying in ones house was a risk factor for contracting malaria (OR = 1, 68 CI 0, 74-3, 83). This finding was not statistically significant. Sleeping under an insecticidal net and wearing protective clothing when outdoors after dusk were protective factors against contracting malaria (OR = 0, 27 CI 0, 12-0, 59 and OR = 0, 12 CI 0, 06-0, 25 respectively). All cases were treated according to the national malaria case management guidelines.
Risk factors for contracting malaria were being under the age of 5 years, outdoor activities at night and not using mosquito repellents. Net use was a protective factor from contracting malaria in Mutasa District. Indoor residual spraying with pyrethroids in Honde Valley was not a protective factor against contracting malaria.
2014年1月,津巴布韦穆塔萨区洪德谷地区宣布爆发疟疾疫情。该地区气候炎热、温和,降雨量大,是媒介繁殖和疟疾传播的理想环境。重力灌溉渠道贯穿山谷,为疟疾媒介蚊子创造了许多繁殖场所。尽管该地区已实现诸如使用拟除虫菊酯进行室内滞留喷洒(IRS)和分发长效驱虫蚊帐等预防干预措施的既定目标,但在过去几年中疟疾疫情仍屡见不鲜。本研究的目的是按人、地点和时间描述疫情,评估社区对疟疾传播、体征和症状以及治疗的了解,并找出该地区与疟疾感染相关的因素。
开展了一项非匹配病例对照研究。对符合纳入标准的山谷居民进行访谈式问卷调查,以找出可能与疟疾感染相关的因素。病例定义为2014年1月13日至1月26日期间有疟疾症状且确诊的洪德谷居民。对照为疫情期间在穆塔萨区但未出现疟疾症状的居民。共纳入87例病例和87名对照。
病例组和对照组在社会人口学特征以及对疟疾传播、治疗和预防的了解方面具有可比性。疫情期间感染疟疾的危险因素包括5岁以下(比值比[OR]=9.92,可信区间[CI]1.2 - 80.1)、未使用驱蚊剂(OR = 8.25,CI 3.78 - 18.0)、黎明前和黄昏后进行户外活动(OR = 2.81,CI 1.04 - 7.6)。家中接受过室内滞留喷洒是感染疟疾的危险因素(OR = 1.68,CI 0.74 - 3.83)。这一发现无统计学意义。在驱虫蚊帐下睡觉以及黄昏后户外活动时穿着防护服是预防感染疟疾的保护因素(分别为OR = 0.27,CI 0.12 - 0.59和OR = 0.12,CI 0.06 - 0.25)。所有病例均按照国家疟疾病例管理指南进行治疗。
感染疟疾的危险因素包括5岁以下、夜间户外活动以及未使用驱蚊剂。使用蚊帐是穆塔萨区预防感染疟疾的保护因素。在洪德谷使用拟除虫菊酯进行室内滞留喷洒并非预防感染疟疾的保护因素。