Department of Primary Health Care Sciences, Global and Public Health Unit, University of Zimbabwe, Harare, Zimbabwe.
Provincial Medical Directorate, Zimbabwe Ministry of Health and Child Care, Manicaland , Zimbabwe.
Malar J. 2022 Mar 19;21(1):94. doi: 10.1186/s12936-022-04106-9.
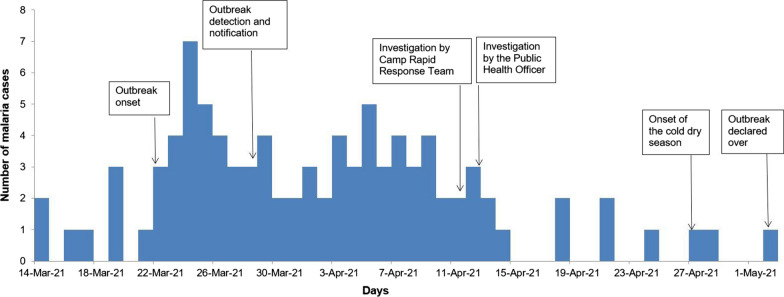
Malaria is a leading cause of morbidity and mortality among forcibly displaced populations, including refugees, approximately two-thirds of whom reside in malaria endemic regions. Data from the rapid disease notification system (RDNS) reports for Manicaland Province in Zimbabwe showed that despite implementation of malaria control initiatives, there was an increase in number of malaria cases above action thresholds at Tongogara refugee camp in Chipinge district during weeks 12-14 of 2021. An investigation that described the outbreak by person, place and time was conducted. Malaria emergency preparedness, response, and appropriateness of case management were assessed. The factors associated with contracting malaria were determined to enable the formulation of appropriate interventions, establish control, and prevent future malaria outbreaks among this vulnerable population.
A 1:1 unmatched case-control study involving 80 cases and 80 controls was conducted using interviewer-administered questionnaires at household level. Data was entered into Epi Data version 3.1 and quantitative analysis was done using Epi Info™ version 7.2.2.6 to generate medians, proportions, odds ratios and their 95% confidence intervals.
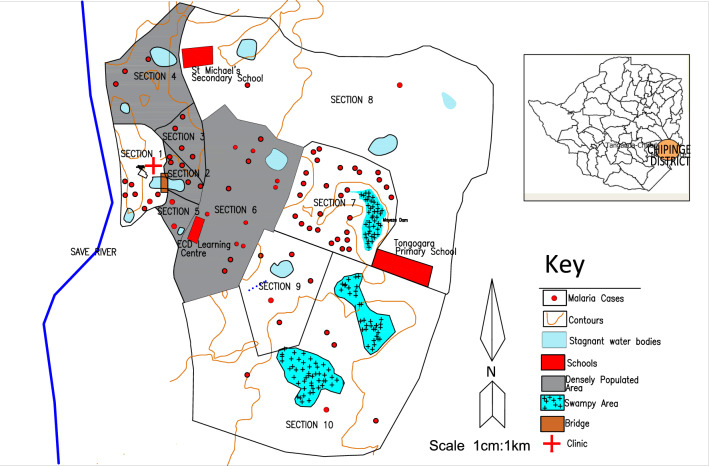
Malaria cases were distributed throughout the 10 residential sections within Tongogara refugee camp, the majority being from section 7, 28 (35%). Despite constituting 11% of the total population, Mozambican nationals accounted for 36 (45%) cases. Males constituted 47 (59%) among cases which was comparable to controls 43 (54%), p = 0.524. The median age for cases was 15 years [Interquartile range (IQR), 9-26] comparable to controls, which was 17 years (IQR, 10-30) (p = 0.755). Several natural and man-made potential vector breeding sites were observed around the camp. Risk factors associated with contracting malaria were engaging in outdoor activities at night [AOR = 2.74 (95% CI 1.04-7.22), wearing clothes that do not cover the whole body during outdoor activities [AOR 4.26 (95% CI, 1.43-12.68)], while residing in a refugee housing unit reduced the risk of contracting malaria [AOR = 0.18 (CI, 0.06-0.55)].
The malaria outbreak at Tongogara refugee camp reemphasizes the role of behavioural factors in malaria transmission. Intensified health education to address human behaviours that expose residents to malaria, habitat modification, and larviciding to eliminate mosquito breeding sites were recommended.
疟疾是导致被迫流离失所人群(包括难民)发病率和死亡率的主要原因,其中约三分之二的难民居住在疟疾流行地区。津巴布韦马尼卡兰省快速疾病通报系统(RDNS)的数据显示,尽管实施了疟疾控制措施,但在 2021 年第 12-14 周期间,奇平格区 Tongogara 难民营的疟疾病例数超过了行动阈值。对此进行了一次描述暴发的人与地点时间的调查。评估了疟疾应急准备、应对和病例管理的适当性。确定了与疟疾相关的发病因素,以便制定适当的干预措施,建立控制,并防止这一脆弱人群中未来的疟疾暴发。
采用 1:1 不匹配病例对照研究,在家庭层面上对 80 例病例和 80 例对照进行访谈式问卷调查。数据输入 Epi Data 版本 3.1,并使用 Epi Info™ 版本 7.2.2.6 进行定量分析,生成中位数、比例、比值比及其 95%置信区间。
疟疾病例分布在 Tongogara 难民营的 10 个居住区内,大多数病例来自第 7 区,有 28 例(35%)。莫桑比克人尽管占总人口的 11%,但占病例的 36 例(45%)。男性病例占 47 例(59%),与对照组的 43 例(54%)相似,p=0.524。病例的中位年龄为 15 岁[四分位距(IQR),9-26],与对照组的 17 岁(IQR,10-30)相似(p=0.755)。在营地周围观察到几个自然和人为的潜在媒介滋生地。与感染疟疾相关的风险因素包括夜间户外活动[比值比(AOR)=2.74(95%置信区间(CI),1.04-7.22)]、户外活动时不穿全身衣服[AOR 4.26(95%CI,1.43-12.68)],而居住在难民住房单元可降低感染疟疾的风险[AOR=0.18(CI,0.06-0.55)]。
Tongogara 难民营的疟疾暴发再次强调了行为因素在疟疾传播中的作用。建议加强卫生教育,解决使居民易患疟疾的行为、栖息地改造和灭蚊幼虫以消除蚊虫滋生地等问题。