Kilburn Jeremy M, Soike Michael H, Lucas John T, Ayala-Peacock Diandra, Blackstock William, Isom Scott, Kearns William T, Hinson William H, Miller Antonius A, Petty William J, Munley Michael T, Urbanic James J
Department of Radiation Oncology, Wake Forest Baptist Health, Winston-Salem, NC.
Department of Radiation Oncology, Wake Forest Baptist Health, Winston-Salem, NC.
Pract Radiat Oncol. 2016 May-Jun;6(3):e73-e80. doi: 10.1016/j.prro.2015.10.004. Epub 2015 Oct 22.
Image guided radiation therapy (IGRT) is designed to ensure accurate and precise targeting, but whether improved clinical outcomes result is unknown.
A retrospective comparison of locally advanced lung cancer patients treated with and without IGRT from 2001 to 2012 was conducted. Median local failure-free survival (LFFS), regional, locoregional failure-free survival (LRFFS), distant failure-free survival, progression-free survival, and overall survival (OS) were estimated. Univariate and multivariate models assessed the association between patient- and treatment-related covariates and local failure.
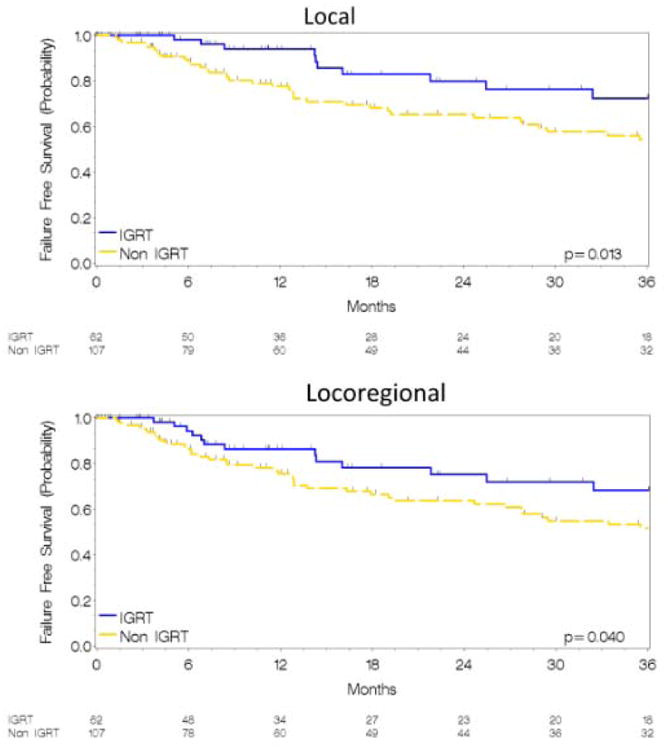
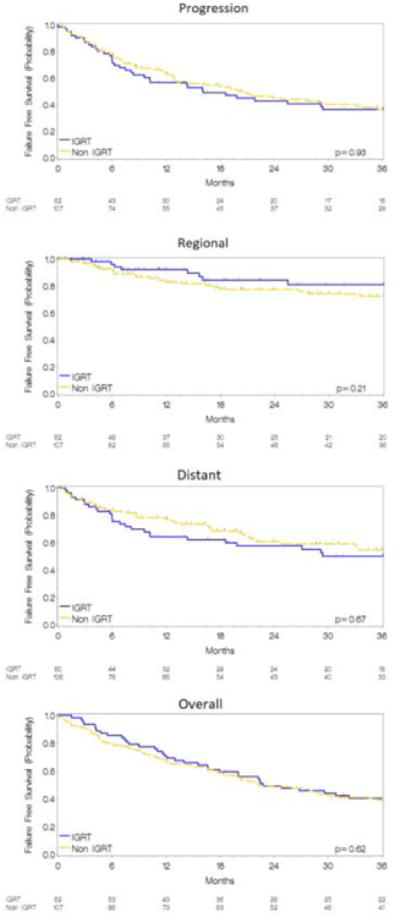
A total of 169 patients were treated with definitive radiation therapy and concurrent chemotherapy with a median follow-up of 48 months in the IGRT cohort and 96 months in the non-IGRT cohort. IGRT was used in 36% (62 patients) of patients. OS was similar between cohorts (2-year OS, 47% vs 49%, P = .63). The IGRT cohort had improved 2-year LFFS (80% vs 64%, P = .013) and LRFFS (75% and 62%, P = .04). Univariate analysis revealed IGRT and treatment year improved LFFS, whereas group stage, dose, and positron emission tomography/computed tomography planning had no impact. IGRT remained significant in the multivariate model with an adjusted hazard ratio of 0.40 (P = .01). Distant failure-free survival (58% vs 59%, P = .67) did not differ significantly.
IGRT with daily cone beam computed tomography confers an improvement in the therapeutic ratio relative to patients treated without this technology.
图像引导放射治疗(IGRT)旨在确保精确靶向,但能否改善临床结果尚不清楚。
对2001年至2012年接受或未接受IGRT治疗的局部晚期肺癌患者进行回顾性比较。估计中位无局部失败生存期(LFFS)、区域、局部区域无失败生存期(LRFFS)、无远处失败生存期、无进展生存期和总生存期(OS)。单变量和多变量模型评估患者和治疗相关协变量与局部失败之间的关联。
共有169例患者接受了根治性放疗和同步化疗,IGRT队列的中位随访时间为48个月,非IGRT队列的中位随访时间为96个月。36%(62例)的患者使用了IGRT。队列之间的OS相似(2年OS,47%对49%,P = 0.63)。IGRT队列的2年LFFS有所改善(80%对64%,P = 0.013),LRFFS也有所改善(75%和62%,P = 0.04)。单变量分析显示IGRT和治疗年份改善了LFFS,而组分期、剂量和正电子发射断层扫描/计算机断层扫描计划没有影响。在多变量模型中,IGRT仍然显著,调整后的风险比为0.40(P = 0.01)。无远处失败生存期(58%对59%,P = 0.67)无显著差异。
与未使用该技术治疗的患者相比,每日锥形束计算机断层扫描的IGRT提高了治疗比率。