Chang Warren, Pope Whitney B, Harris Robert J, Hardy Anthony J, Leu Kevin, Mody Reema R, Nghiemphu Phioanh L, Lai Albert, Cloughesy Timothy F, Ellingson Benjamin M
Dept. of Radiological Sciences, David Geffen School of Medicine at UCLA.
Dept. of Radiological Sciences, David Geffen School of Medicine at UCLA; Dept. of Biomedical Physics, David Geffen School of Medicine at UCLA.
Tomography. 2015 Sep;1(1):37-43. doi: 10.18383/j.tom.2015.00115.
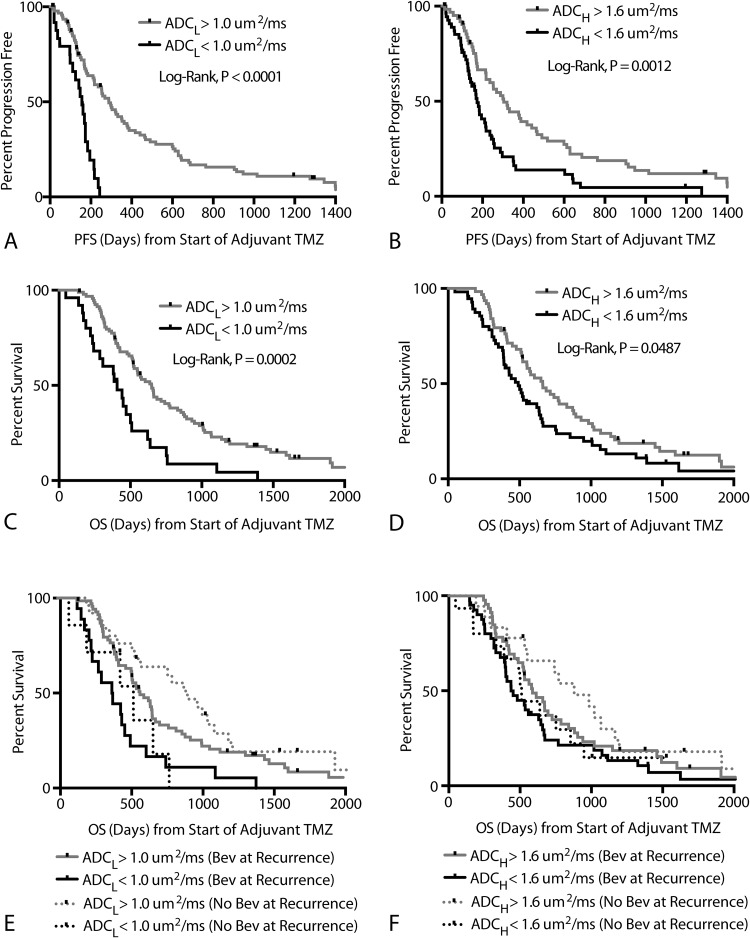
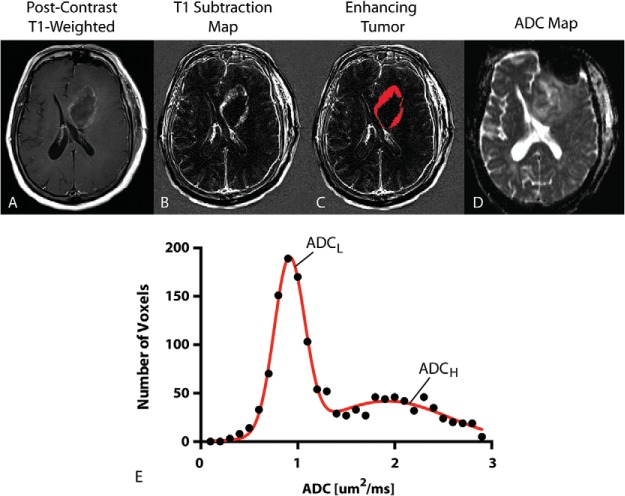
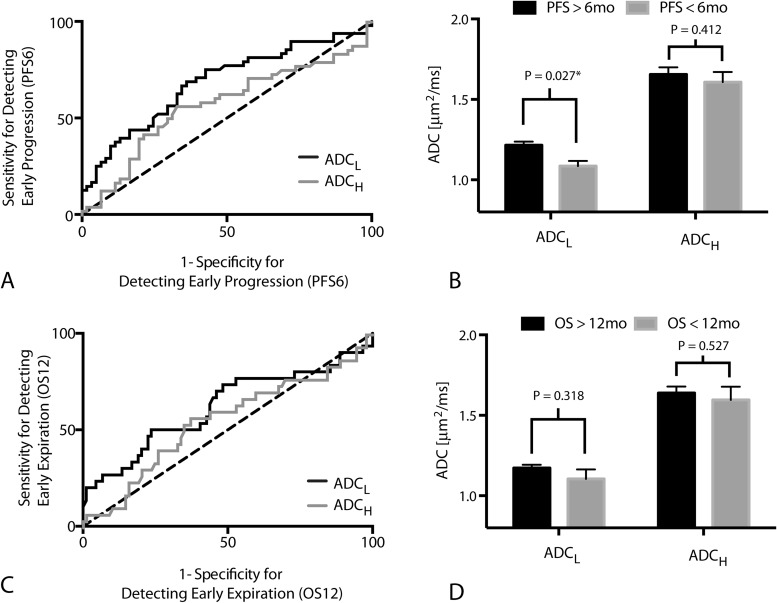
The standard of care for newly diagnosed glioblastoma (GBM) is surgery, then radiotherapy (RT) with concurrent temozolomide (TMZ), followed by adjuvant TMZ. We hypothesized patients with low diffusivity measured using apparent diffusion coefficient (ADC) histogram analysis evaluated after RT+TMZ, prior to adjuvant TMZ, would have a significantly shorter progression-free (PFS) and overall survival (OS). To test this hypothesis we evaluated 120 patients with newly diagnosed GBM receiving RT+TMZ followed by adjuvant TMZ. MRI was performed after completion of RT+TMZ, prior to initiation of adjuvant TMZ. A double Gaussian mixed model was used to describe the ADC histograms within the enhancing tumor, where ADC and ADC were defined as the mean ADC value of the lower and higher Gaussian distribution, respectively. An ADC value of 1.0 um/ms and ADC value of 1.6 um/ms were used to stratify patients into high and low risk categories. Results suggest patients with low ADC had significantly shorter PFS (Cox Hazard Ratio = 0.12, P = 0.0006). OS was significantly shorter with low ADC tumors, showing a median OS of 407 vs. 644 days (Cox Hazard Ratio = 0.31, P = 0.047). ADC was not predictive of PFS or OS when accounting for age and ADC. In summary, newly diagnosed glioblastoma patients with low ADC after completion of RT+TMZ are likely to progress and die earlier than patients with higher ADC. Results suggest ADC histogram analysis may be useful for patient risk stratification following completion of RT+TMZ.
新诊断胶质母细胞瘤(GBM)的标准治疗方案是手术,然后进行放疗(RT)并同步使用替莫唑胺(TMZ),随后进行辅助性TMZ治疗。我们假设,在RT + TMZ治疗后、辅助性TMZ治疗前,通过表观扩散系数(ADC)直方图分析测量出扩散率较低的患者,其无进展生存期(PFS)和总生存期(OS)会显著缩短。为验证这一假设,我们评估了120例接受RT + TMZ治疗后再进行辅助性TMZ治疗的新诊断GBM患者。在RT + TMZ治疗完成后、辅助性TMZ治疗开始前进行了MRI检查。采用双高斯混合模型描述增强肿瘤内的ADC直方图,其中ADC₁和ADC₂分别定义为较低和较高高斯分布的平均ADC值。使用1.0 um²/ms的ADC值和1.6 um²/ms的ADC值将患者分为高风险和低风险类别。结果表明,ADC值低的患者PFS显著缩短(Cox风险比 = 0.12,P = 0.0006)。ADC值低的肿瘤患者OS显著缩短,中位OS为407天对644天(Cox风险比 = 0.31,P = 0.047)。在考虑年龄和ADC₁时,ADC₂不能预测PFS或OS。总之,RT + TMZ治疗完成后ADC值低的新诊断胶质母细胞瘤患者比ADC值高的患者更易进展且死亡更早。结果表明,ADC直方图分析可能有助于RT + TMZ治疗完成后的患者风险分层。