Shields Lisa B E, Shelton Brent J, Shearer Andrew J, Chen Li, Sun David A, Parsons Sarah, Bourne T David, LaRocca Renato, Spalding Aaron C
Norton Neuroscience Institute, Norton Healthcare, Louisville, KY, USA.
The Brain Tumor Center, Norton Healthcare, Louisville, KY, USA.
Radiat Oncol. 2015 Oct 31;10:222. doi: 10.1186/s13014-015-0527-0.
Dexamethasone (DXM) is commonly used in the management of cerebral edema in patients diagnosed with glioblastoma multiforme (GBM). Bevacizumab (BEV) is FDA-approved for the progression or recurrence of GBM but has not been shown to improve survival when given for newly diagnosed patients concurrently with radiation (RT) and temozolomide (TMZ). Both DXM and BEV reduce cerebral edema, however, DXM has been shown to induce cytokine cascades which could interfere with cytotoxic therapy. We investigated whether DXM would reduce survival of GBM patients in the setting of concurrent TMZ and BEV administration.
We reviewed the treatment of all 73 patients with GBM who received definitive therapy at our institution from 2005 to 2013 with RT (60 Gy) delivered with concurrent daily TMZ (75 mg/m(2)). Of these, 34 patients also were treated with concurrent BEV (10 mg/kg every two weeks). Patients received adjuvant therapy (TMZ or TMZ/Bev) until either progression, discontinuation due to toxicity, or 12 months after radiation completion. All patients who had GBM progression with TMZ were offered BEV for salvage therapy, with 19 (56 %) receiving BEV.
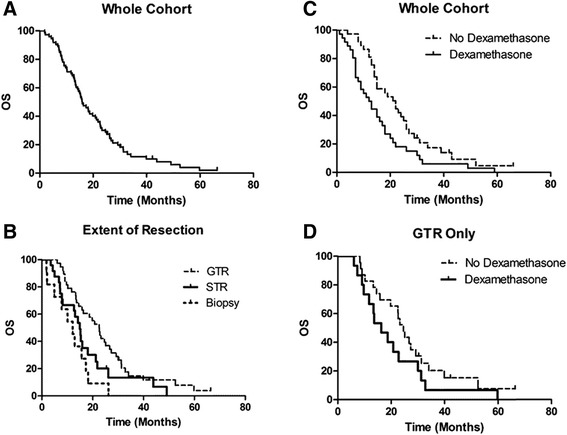
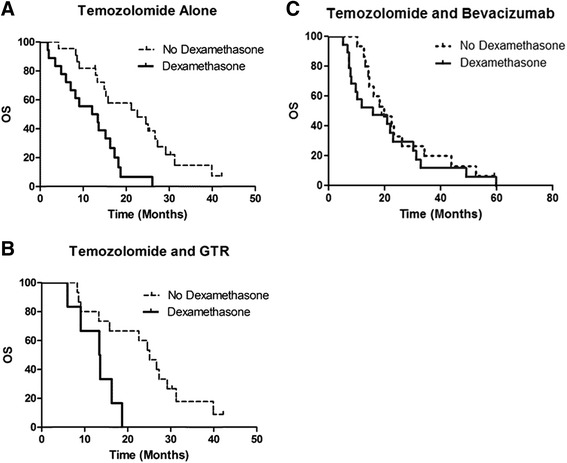
With a median follow-up of 15.6 months, 67 (91.8 %) patients were deceased. The OS for the entire cohort was 15.9 months, while the PFS was 7.7 months. The extent of resection was a prognostic indicator for OS (p = .0044). The median survival following gross tumor resection (GTR) was 22.5 months, subtotal resection (STR) was 14.9 months, and biopsy was 12.1 months. The addition of BEV to TMZ with RT was borderline significantly associated with increased PFS (9.4 vs. 5.1 months, p = 0.0574) although was not significantly associated with OS (18.1 vs. 15.3 months respectively, p = 0.3064). In patients receiving TMZ, DXM use concurrent with RT was a poor prognostic indicator of both OS (12.7 vs. 22.6 months, p = 0.003) and PFS (3.6 vs. 8.4 months, p <0.0001). DXM did not reduce OS in patients who received TMZ and BEV concurrently with RT (22.9 vs 22.8 months, p = 0.4818). On multivariable analysis, DXM use predicted an unfavorable OS hazard ratio (HR) = 1.72, p = 0.045).
Our results with TMZ, BEV, and RT are similar to previous studies in terms of PFS and OS. DXM use during RT with concurrent TMZ correlated with reduced OS and PFS unless BEV was administered.
地塞米松(DXM)常用于多形性胶质母细胞瘤(GBM)患者脑水肿的治疗。贝伐单抗(BEV)已获美国食品药品监督管理局(FDA)批准用于GBM进展或复发的治疗,但对于新诊断患者,在与放疗(RT)及替莫唑胺(TMZ)联合使用时,尚未显示出能提高生存率。DXM和BEV均可减轻脑水肿,然而,DXM已被证明可诱导细胞因子级联反应,这可能会干扰细胞毒性治疗。我们研究了在同时给予TMZ和BEV的情况下,DXM是否会降低GBM患者的生存率。
我们回顾了2005年至2013年在我们机构接受确定性治疗的所有73例GBM患者的治疗情况,这些患者接受了RT(60 Gy)并同时每日给予TMZ(75 mg/m²)。其中,34例患者还同时接受了BEV治疗(每两周10 mg/kg)。患者接受辅助治疗(TMZ或TMZ/贝伐单抗),直至疾病进展、因毒性而停药或放疗结束后12个月。所有TMZ治疗后出现GBM进展的患者均接受BEV挽救治疗,其中19例(56%)接受了BEV治疗。
中位随访15.6个月,67例(91.8%)患者死亡。整个队列的总生存期(OS)为15.9个月,无进展生存期(PFS)为7.7个月。切除范围是OS的一个预后指标(p = 0.0044)。大体肿瘤切除(GTR)后的中位生存期为22.5个月,次全切除(STR)为14.9个月,活检为12.1个月。RT联合TMZ时加用BEV与PFS增加有边缘显著相关性(9.4个月对5.1个月,p = 0.0574),但与OS无显著相关性(分别为18.1个月对15.3个月,p = 0.3064)。在接受TMZ治疗的患者中,RT时同时使用DXM是OS(12.7个月对22.6个月,p = 0.003)和PFS(3.6个月对8.4个月,p <0.0001)的不良预后指标。在RT时同时接受TMZ和BEV的患者中,DXM并未降低OS(22.9个月对22.8个月,p = 0.4818)。多变量分析显示,使用DXM预测不良OS风险比(HR)= 1.72,p = 0.045)。
我们使用TMZ、BEV和RT的结果在PFS和OS方面与先前的研究相似。RT时同时使用TMZ时使用DXM与OS和PFS降低相关,除非给予BEV。