Oster Matthew E, Kelleman Michael, McCracken Courtney, Ohye Richard G, Mahle William T
Children's Healthcare of Atlanta, GA (M.E.O., W.T.M.) Emory University School of Medicine, Atlanta, GA (M.E.O., M.K., C.M.C., W.T.M.).
Emory University School of Medicine, Atlanta, GA (M.E.O., M.K., C.M.C., W.T.M.).
J Am Heart Assoc. 2016 Jan 13;5(1):e002566. doi: 10.1161/JAHA.115.002566.
Mortality for infants with single ventricle congenital heart disease remains as high as 8% to 12% during the interstage period, the time between discharge after the Norwood procedure and before the stage II palliation. The objective of our study was to determine the association between digoxin use and interstage mortality in these infants.
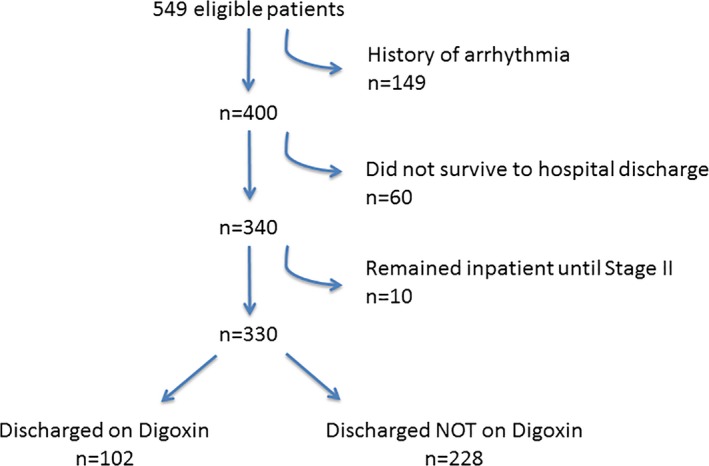
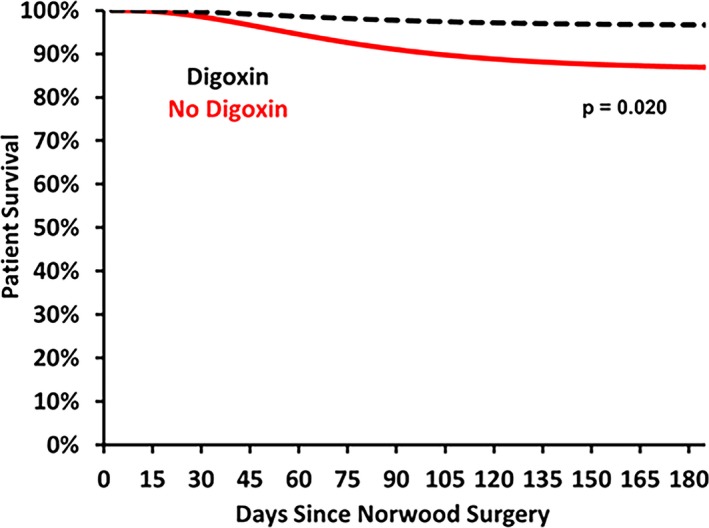
We conducted a retrospective cohort study using the Pediatric Heart Network Single Ventricle Reconstruction Trial public use dataset, which includes data on infants with single right ventricle congenital heart disease randomized to receive either a Blalock-Taussig shunt or right ventricle-to-pulmonary artery shunt during the Norwood procedure at 15 institutions in North America from 2005 to 2008. Parametric survival models were used to compare the risk of interstage mortality between those discharged to home on digoxin versus those discharged to home not on digoxin, adjusting for center volume, ascending aorta diameter, shunt type, and socioeconomic status. Of the 330 infants eligible for this study, 102 (31%) were discharged home on digoxin. Interstage mortality for those not on digoxin was 12.3%, compared to 2.9% among those on digoxin, with an adjusted hazard ratio of 3.5 (95% CI, 1.1-11.7; P=0.04). The number needed to treat to prevent 1 death was 11 patients. There were no differences in complications between the 2 groups during the interstage period.
Digoxin use in infants with single ventricle congenital heart disease is associated with significantly reduced interstage mortality.
单心室先天性心脏病婴儿在过渡期(即诺伍德手术后出院至二期姑息治疗前这段时间)的死亡率仍高达8%至12%。我们研究的目的是确定这些婴儿使用地高辛与过渡期死亡率之间的关联。
我们使用儿科心脏网络单心室重建试验公共使用数据集进行了一项回顾性队列研究,该数据集包含2005年至2008年在北美15家机构接受诺伍德手术时被随机分配接受布莱洛克 - 陶西格分流术或右心室至肺动脉分流术的单右心室先天性心脏病婴儿的数据。使用参数生存模型比较出院时服用地高辛与未服用地高辛的婴儿之间的过渡期死亡风险,并对中心容量、升主动脉直径、分流类型和社会经济状况进行调整。在符合本研究条件的330名婴儿中,102名(31%)出院时服用地高辛。未服用地高辛的婴儿过渡期死亡率为12.3%,而服用地高辛的婴儿为2.9%,调整后的风险比为3.5(95%CI,1.1 - 11.7;P = 0.04)。预防1例死亡所需治疗的患者数为11名。两组在过渡期的并发症无差异。
单心室先天性心脏病婴儿使用地高辛与显著降低过渡期死亡率相关。