Marsh Elisabeth B, Llinas Rafael H, Schneider Andrea L C, Hillis Argye E, Lawrence Erin, Dziedzic Peter, Gottesman Rebecca F
From the Johns Hopkins School of Medicine, Department of Neurology (EBM, RHL, AEH, PD, RFG); Johns Hopkins Bayview Medical Center (EBM, RHL, EL, RFG); and Johns Hopkins Bloomberg School of Public Health, Department of Epidemiology, Baltimore, MD, USA (ALCS, RFG).
Medicine (Baltimore). 2016 Jan;95(2):e2430. doi: 10.1097/MD.0000000000002430.
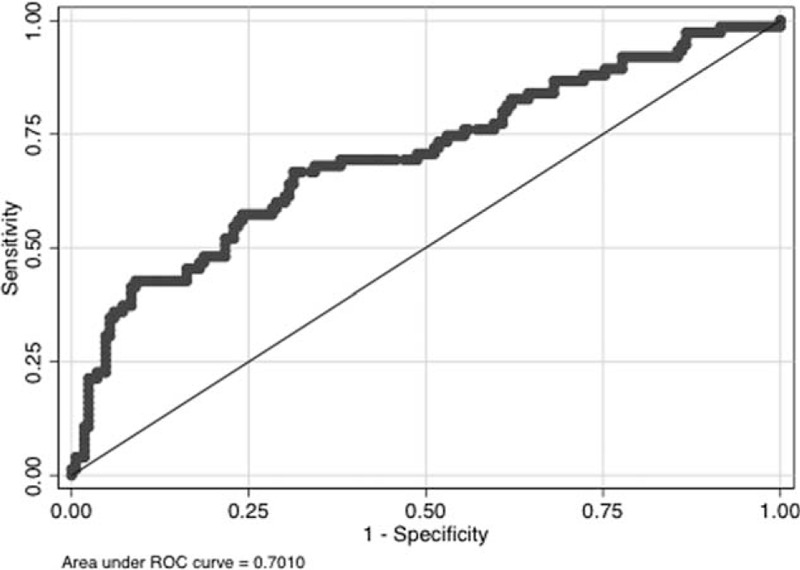
Hemorrhagic transformation (HT) increases the morbidity and mortality of ischemic stroke. Anticoagulation is often indicated in patients with atrial fibrillation, low ejection fraction, or mechanical valves who are hospitalized with acute stroke, but increases the risk of HT. Risk quantification would be useful. Prior studies have investigated risk of systemic hemorrhage in anticoagulated patients, but none looked specifically at HT. In our previously published work, age, infarct volume, and estimated glomerular filtration rate (eGFR) significantly predicted HT. We created the hemorrhage risk stratification (HeRS) score based on regression coefficients in multivariable modeling and now determine its validity in a prospectively followed inpatient cohort.A total of 241 consecutive patients presenting to 2 academic stroke centers with acute ischemic stroke and an indication for anticoagulation over a 2.75-year period were included. Neuroimaging was evaluated for infarct volume and HT. Hemorrhages were classified as symptomatic versus asymptomatic, and by severity. HeRS scores were calculated for each patient and compared to actual hemorrhage status using receiver operating curve analysis.Area under the curve (AUC) comparing predicted odds of hemorrhage (HeRS score) to actual hemorrhage status was 0.701. Serum glucose (P < 0.001), white blood cell count (P < 0.001), and warfarin use prior to admission (P = 0.002) were also associated with HT in the validation cohort. With these variables, AUC improved to 0.854. Anticoagulation did not significantly increase HT; but with higher intensity anticoagulation, hemorrhages were more likely to be symptomatic and more severe.The HeRS score is a valid predictor of HT in patients with ischemic stroke and indication for anticoagulation.
出血性转化(HT)会增加缺血性卒中的发病率和死亡率。对于因急性卒中住院的心房颤动、射血分数低或有机械瓣膜的患者,通常需要进行抗凝治疗,但这会增加HT的风险。风险量化将很有用。先前的研究调查了抗凝患者发生全身性出血的风险,但没有一项专门针对HT进行研究。在我们之前发表的研究中,年龄、梗死体积和估计肾小球滤过率(eGFR)是HT的显著预测因素。我们基于多变量模型中的回归系数创建了出血风险分层(HeRS)评分,现在在前瞻性随访的住院患者队列中确定其有效性。
在2.75年的时间里,共有241例连续就诊于2个学术性卒中中心、患有急性缺血性卒中且有抗凝指征的患者被纳入研究。对神经影像学进行评估以确定梗死体积和HT情况。出血被分为有症状与无症状,并根据严重程度进行分类。为每位患者计算HeRS评分,并使用受试者工作特征曲线分析将其与实际出血状态进行比较。
将预测出血几率(HeRS评分)与实际出血状态进行比较的曲线下面积(AUC)为0.701。在验证队列中,血清葡萄糖(P<0.001)、白细胞计数(P<0.001)和入院前使用华法林(P=0.002)也与HT相关。纳入这些变量后,AUC提高到了0.854。抗凝治疗并没有显著增加HT的发生;但抗凝强度越高,出血越有可能有症状且更严重。
HeRS评分是有缺血性卒中和抗凝指征患者HT的有效预测指标。