Department of Neurology University Medical Center Groningen Groningen The Netherlands; Institute of Psychological Medicine and Clinical Neurosciences MRC Centre for Neuropsychiatric Genetics and Genomics Cardiff University Cardiff United Kingdom.
Department of Neurology The Academic Medical Center Amsterdam The Netherlands.
Ann Clin Transl Neurol. 2015 Nov 20;3(1):4-11. doi: 10.1002/acn3.263. eCollection 2016 Jan.
Myoclonus-dystonia (M-D) is a hyperkinetic movement disorder, typically alcohol-responsive upper body myoclonus and dystonia. The majority of autosomal dominant familial cases are caused by epsilon-sarcoglycan gene (SGCE) mutations. Previous publications have observed increased rates of psychiatric disorders amongst SGCE mutation-positive populations. We analyzed the psychiatric data from four international centers, forming the largest cohort to date, to further determine the extent and type of psychiatric disorders in M-D.
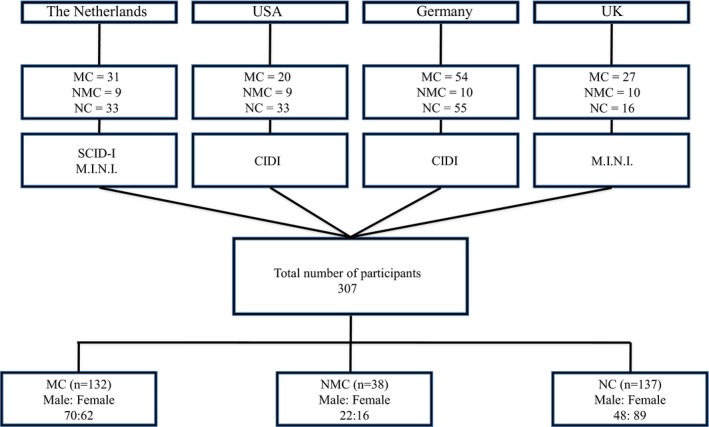
Psychiatric data from SGCE mutation-positive M-D cohorts, collected by movement disorder specialists in the Netherlands, United Kingdom, United States, and Germany, were analyzed. These data were collected using standardized, systematic questionnaires allowing classification of symptoms according to Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria. Based on motor findings and SGCE mutation analysis, participants were classified into one of three groups: manifesting carriers, nonmanifesting carriers and noncarriers.
Data from 307 participants were evaluated (140 males, 167 females, mean age at examination: 42.5 years). Two-thirds of motor affected mutation carriers (n = 132) had ≥1 psychiatric diagnosis, specific, and social phobias being most common followed by alcohol dependence and obsessive-compulsive disorder (OCD). Compared to familial controls, affected mutation carriers had significantly elevated overall rates of psychiatric disorders (P < 0.001). The most significant differences were observed with alcohol dependence (P < 0.001), OCD (P < 0.001), social and specific phobias (P < 0.001).
M-D due to SGCE mutations is associated with specific psychiatric disorders, most commonly OCD, anxiety-related disorders, and alcohol dependence. These suggest either a potential pleiotropic function for SGCE within the central nervous system or a secondary effect of the motor disorder.
肌阵挛-肌张力障碍(M-D)是一种运动障碍,通常表现为酒精反应性上半身肌阵挛和肌张力障碍。大多数常染色体显性家族性病例是由ε-肌聚糖基因(SGCE)突变引起的。以前的出版物观察到 SGCE 突变阳性人群中精神障碍的发生率增加。我们分析了来自四个国际中心的精神科数据,这是迄今为止最大的队列,以进一步确定 M-D 中精神障碍的程度和类型。
对荷兰、英国、美国和德国的运动障碍专家收集的 SGCE 突变阳性 M-D 队列的精神科数据进行了分析。这些数据是使用标准化、系统的问卷收集的,允许根据《精神障碍诊断与统计手册》第四版(DSM-IV)标准对症状进行分类。根据运动表现和 SGCE 突变分析,参与者被分为以下三组之一:表现型携带者、非表现型携带者和非携带者。
对 307 名参与者的数据进行了评估(男性 140 名,女性 167 名,检查时的平均年龄为 42.5 岁)。三分之二的运动受影响的突变携带者(n = 132)有≥1 种精神科诊断,最常见的是特定性和社交恐惧症,其次是酒精依赖和强迫症(OCD)。与家族性对照相比,受影响的突变携带者的精神障碍总体发生率显著升高(P < 0.001)。观察到的最显著差异是酒精依赖(P < 0.001)、强迫症(P < 0.001)、社交和特定性恐惧症(P < 0.001)。
由 SGCE 突变引起的 M-D 与特定的精神障碍有关,最常见的是强迫症、焦虑相关障碍和酒精依赖。这表明 SGCE 在中枢神经系统中可能具有潜在的多效性功能,或者是运动障碍的继发效应。