Hong Sook-Hee, Kim Yeon-Sil, Lee Ji Eun, Kim In-Ho, Kim Seung Joon, Han Daehee, Yoo Ie Ryung, Chung Yang-Guk, Kim Young-Hoon, Lee Kyo-Young, Kang Jin-Hyoung
Division of Medical Oncology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
Cancer Research Institute, The Catholic University of Korea, Seoul, Korea.
Cancer Res Treat. 2016 Jul;48(3):1110-9. doi: 10.4143/crt.2015.289. Epub 2016 Jan 6.
The aim of this study was to analyze clinical characteristics of skeletal metastasis in epidermal growth factor receptor (EGFR) mutant non-small cell lung cancer (NSCLC) and treatment outcomes of continued EGFR tyrosine kinase inhibitor (TKI) therapy in patients presenting with skeletal metastasis progression.
Of the 216 patients treated with EGFR-TKI for management of stage III-IV NSCLC between 2006 and 2012 in Seoul St. Mary's Hospital, 76 patients with confirmed EGFR-mutated NSCLC with skeletal metastases during therapy were analyzed retrospectively.
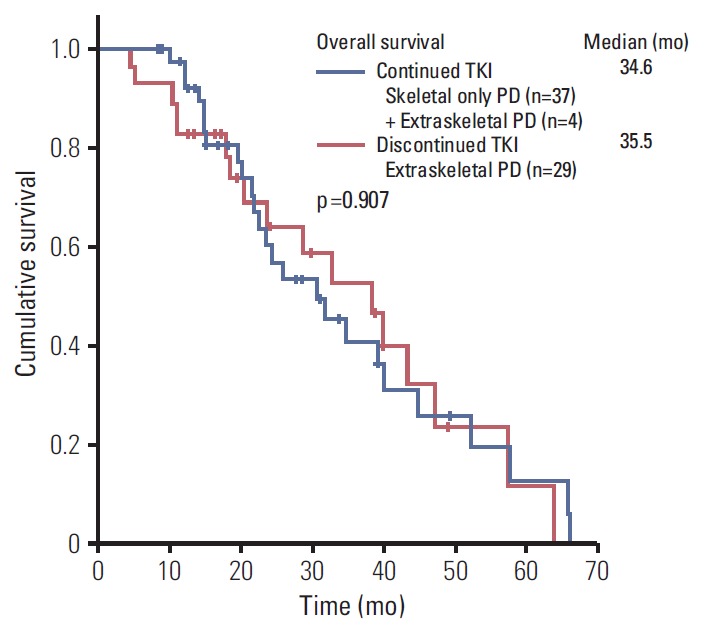
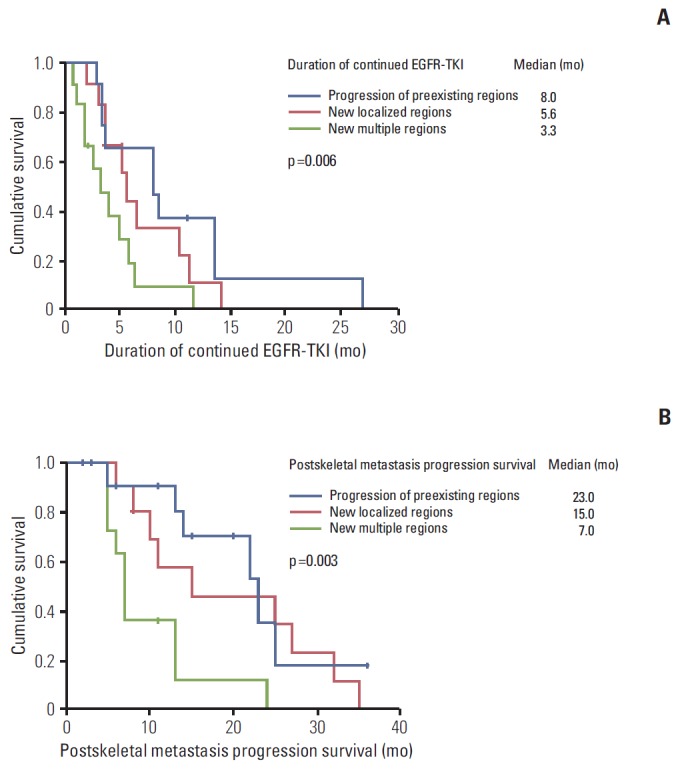
Of 76 patients with EGFR mutant lung cancer with skeletal metastasis, 37 patients developed first progressive disease (PD) in skeletal regions. EGFR-TKI was continued in these 37 patients after first PD in skeletal regions. Median time to first PD of skeletal regions was 8.9 months (95% confidence interval [CI], 4.8 to 13.0). Median time of continued EGFR-TKI after first PD of skeletal regions was 8.0 months (95% CI, 2.9 to 13.0) in patients with disease progression of preexisting regions, 5.6 months (95% CI, 4.5 to 6.7) in patients showing new localized regions, and 3.3 months (95% CI, 1.1 to 5.5) in patients with multiple new metastatic regions (p=0.006). Median time of postskeletal metastasis progression survival was 23.0 months (95% CI, 13.5 to 32.5), 15.0 months (95% CI, 3 to 34.7), and 7.0 months (95% CI, 6.0 to 8.0) (p=0.004) in the above described patient groups, respectively. Overall, seven patients (18.9%) had more than one episode of skeletal progression of disease without extraskeletal PD.
Continued EGFR-TKI treatment with adequate local treatment after progression of skeletal metastasis may be considered for patients who show disease progression in preexisting regions or local progression.
本研究旨在分析表皮生长因子受体(EGFR)突变的非小细胞肺癌(NSCLC)骨转移的临床特征,以及骨转移进展患者继续接受EGFR酪氨酸激酶抑制剂(TKI)治疗的疗效。
回顾性分析2006年至2012年在首尔圣母医院接受EGFR-TKI治疗III-IV期NSCLC的216例患者,其中76例在治疗期间确诊为EGFR突变的NSCLC并发生骨转移。
在76例EGFR突变的肺癌骨转移患者中,37例在骨骼区域出现首次疾病进展(PD)。这37例患者在骨骼区域首次PD后继续接受EGFR-TKI治疗。骨骼区域首次PD的中位时间为8.9个月(95%置信区间[CI],4.8至13.0)。在原有区域疾病进展的患者中,骨骼区域首次PD后继续使用EGFR-TKI的中位时间为8.0个月(95%CI,2.9至13.0),出现新的局部区域的患者为5.6个月(95%CI,4.5至6.7),出现多个新转移区域的患者为3.3个月(95%CI,1.1至5.5)(p=0.006)。上述患者组中,骨转移进展后的中位生存时间分别为23.0个月(95%CI,13.5至32.5)、15.0个月(95%CI,3至34.7)和7.0个月(95%CI,6.0至8.0)(p=0.004)。总体而言,7例患者(18.9%)出现不止一次骨转移进展且无骨外PD。
对于原有区域出现疾病进展或局部进展的患者,在骨转移进展后可考虑继续EGFR-TKI治疗并进行适当的局部治疗。