Smith Iain M, James Robert H, Dretzke Janine, Midwinter Mark J
*NIHR Surgical Reconstruction and Microbiology Research Centre, University of Birmingham †Academic Department of Military Surgery and Trauma, Royal Centre for Defence Medicine, ICT Centre, Edgbaston, Birmingham ‡205 (Scottish) Field Hospital, Govan, Glasgow §Academic Department of Military Emergency Medicine, Royal Centre for Defence Medicine, ICT Centre, Edgbaston, Birmingham ||East Anglian Air Ambulance, Gambling Close, Norwich ¶Ministry of Defence Hospital Unit Derriford, Derriford Hospital, Plymouth, United Kingdom **Institute of Applied Health Research, University of Birmingham, Edgbaston, Birmingham, United Kingdom.
Shock. 2016 Jul;46(1):3-16. doi: 10.1097/SHK.0000000000000569.
Administration of high ratios of plasma to packed red blood cells is a routine practice for in-hospital trauma resuscitation. Military and civilian emergency teams are increasingly carrying prehospital blood products (PHBP) for trauma resuscitation. This study systematically reviewed the clinical literature to determine the extent to which the available evidence supports this practice.
Bibliographic databases and other sources were searched to July 2015 using keywords and index terms related to the intervention, setting, and condition. Standard systematic review methodology aimed at minimizing bias was used for study selection, data extraction, and quality assessment (protocol registration
CRD42014013794). Synthesis was mainly narrative with random effects model meta-analysis limited to mortality outcomes.
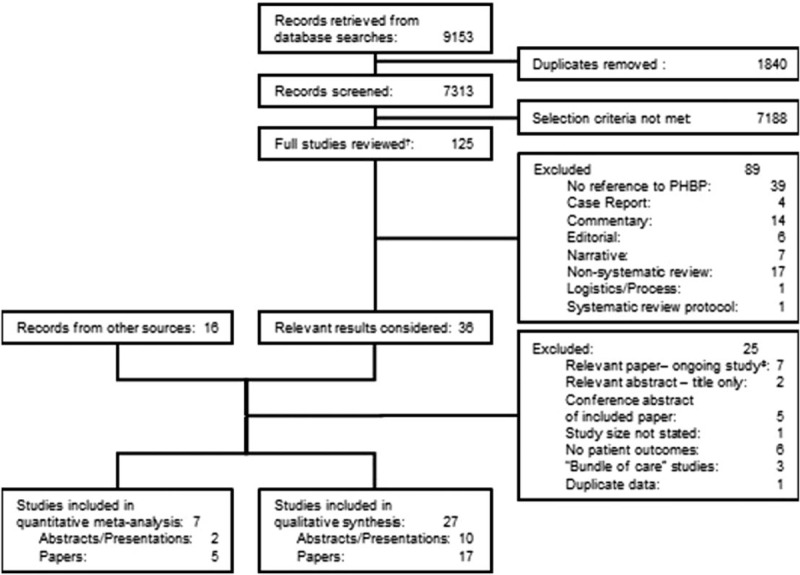
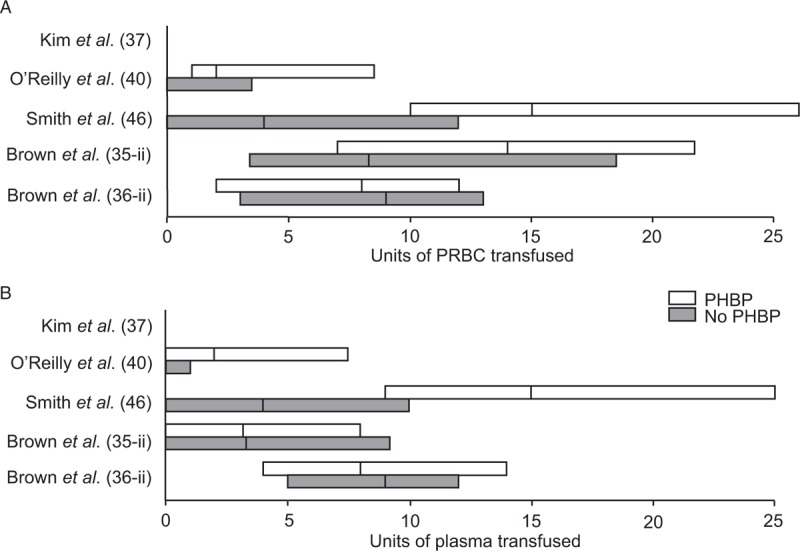
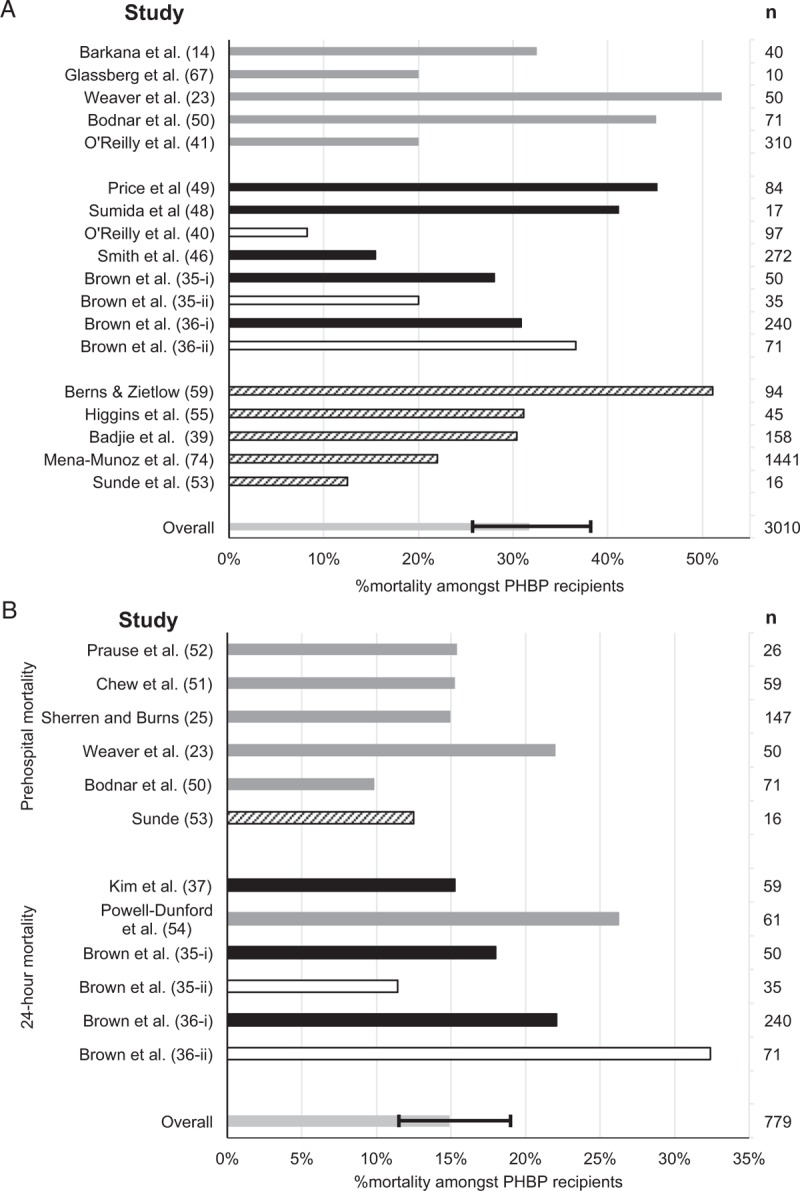
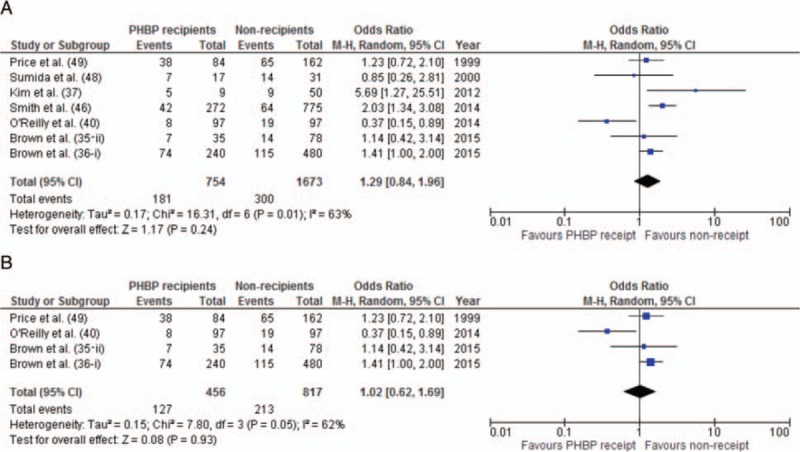
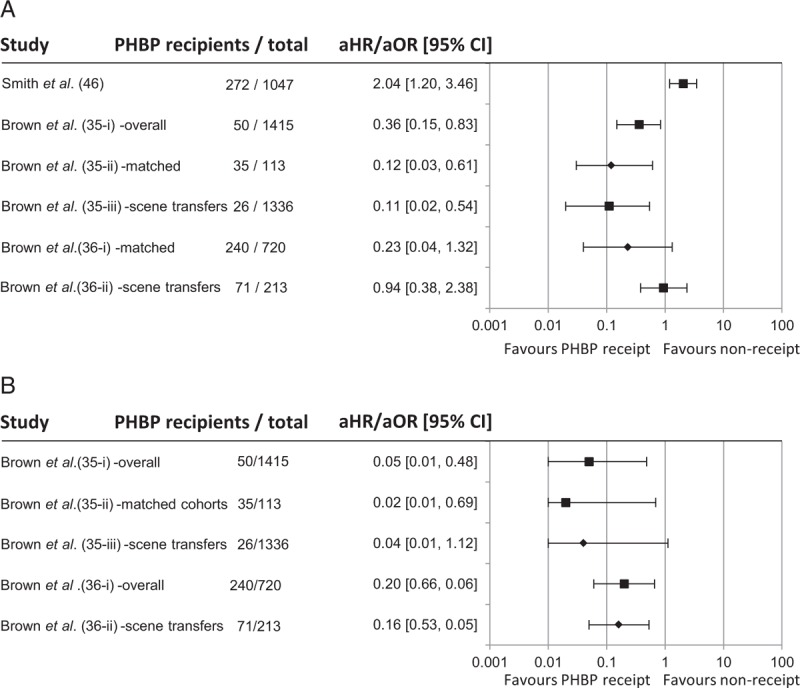
No prospective comparative or randomized studies were identified. Sixteen case series and 11 comparative studies were included in the review. Seven studies included mixed populations of trauma and non-trauma patients. Twenty-five of 27 studies provided only very low quality evidence. No association between PHBP and survival was found (OR for mortality: 1.29, 95% CI: 0.84-1.96, P = 0.24). A single study showed improved survival in the first 24 h. No consistent physiological or biochemical benefit was identified, nor was there evidence of reduced in-hospital transfusion requirements. Transfusion reactions were rare, suggesting the short-term safety of PHBP administration.
While PHBP resuscitation appears logical, the clinical literature is limited, provides only poor quality evidence, and does not demonstrate improved outcomes. No conclusions as to efficacy can be drawn. The results of randomized controlled trials are awaited.
在医院内对创伤患者进行复苏时,采用高比例血浆与浓缩红细胞的输注是常规做法。军事和民用应急团队越来越多地携带院前血液制品(PHBP)用于创伤复苏。本研究系统回顾了临床文献,以确定现有证据支持这种做法的程度。
使用与干预措施、环境和疾病相关的关键词和索引词,检索至2015年7月的文献数据库及其他来源。采用旨在尽量减少偏倚的标准系统评价方法进行研究选择、数据提取和质量评估(方案注册号:PROSPERO:CRD42014013794)。合成主要采用叙述性方法,随机效应模型荟萃分析仅限于死亡率结局。
未检索到前瞻性比较或随机研究。本综述纳入了16个病例系列和11项比较研究。7项研究纳入了创伤和非创伤患者的混合人群。27项研究中有25项仅提供了质量极低的证据。未发现PHBP与生存之间存在关联(死亡率的OR值:1.29,95%CI:0.84 - 1.96,P = 0.24)。一项研究显示在最初24小时内生存率有所提高。未发现一致的生理或生化益处,也没有证据表明住院期间输血需求减少。输血反应很少见,表明输注PHBP具有短期安全性。
虽然PHBP复苏似乎合理,但临床文献有限,仅提供了质量较差的证据,且未显示出改善的结局。无法得出关于疗效的结论。有待随机对照试验的结果。