Wang Li, Lee Myeongjong, Zhang Zhe, Moodie Jessica, Cheng Davy, Martin Janet
Centre for Medical Evidence, Decision Integrity and Clinical Impact (MEDICI), University of Western Ontario, London, Ontario, Canada Chinese Cochrane Centre, West China Hospital, Sichuan University, Chengdu, China Michael G DeGroote Institute for Pain Research and Care, McMaster University, Hamilton, Ontario, Canada.
Department of Anesthesiology and Pain Medicine, Konkuk University School of Medicine, Chungju, South Korea.
BMJ Open. 2016 Feb 2;6(2):e009857. doi: 10.1136/bmjopen-2015-009857.
The clinical impact of preoperative physiotherapy on recovery after joint replacement remains controversial. This systematic review aimed to assess the clinical impact of prehabilitation before joint replacement.
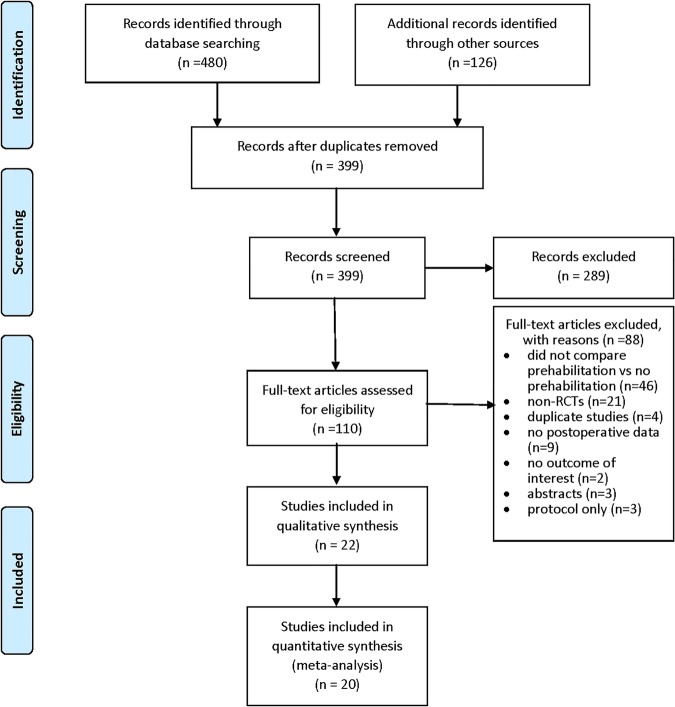
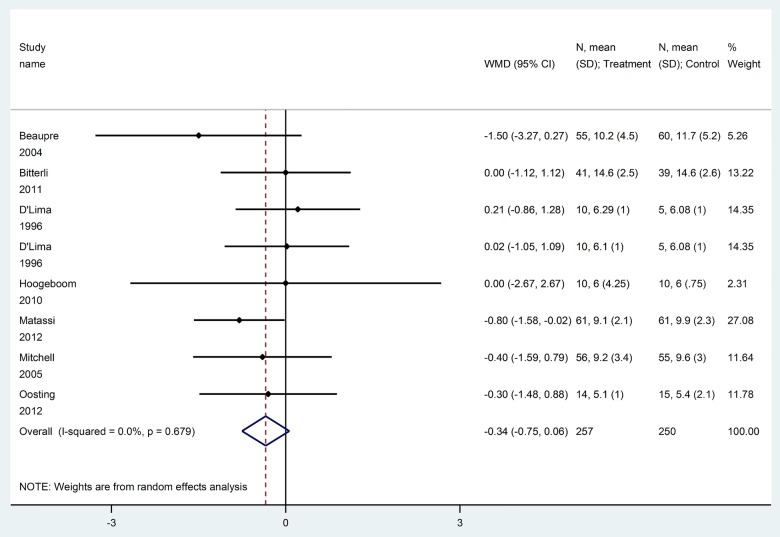
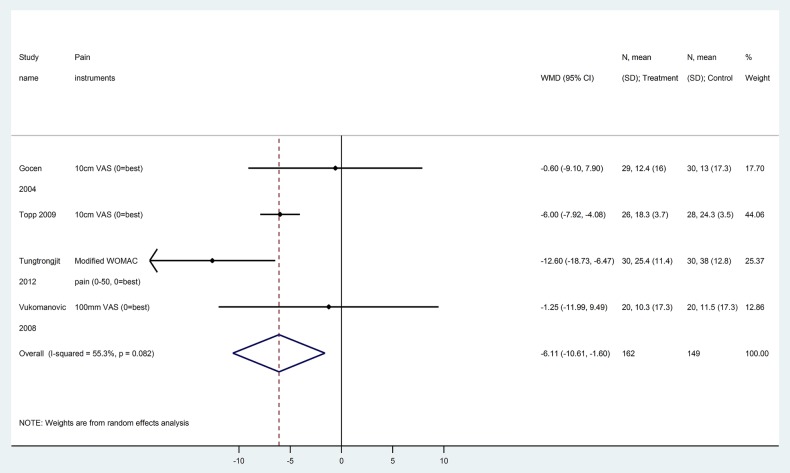
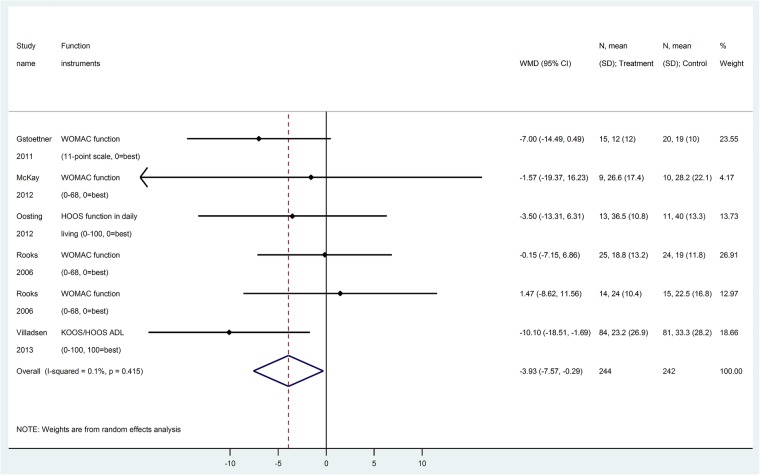
We searched PubMed, Embase and Cochrane CENTRAL up to November 2015 for randomised controlled trials comparing prehabilitation versus no prehabilitation before joint replacement surgery. Postoperative pain and function scores were converted to Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain and function subscales (0-100, high scores indicate worse outcome). Random effects meta-analysis was performed to calculate weighted mean differences (WMD, 95% CI), subgrouped by hip and knee surgery.
Postoperative pain and function scores, time to resume activities of daily living, quality of life, length of hospital stay, total cost, patient satisfaction, postoperative complications, any adverse events and discontinuations.
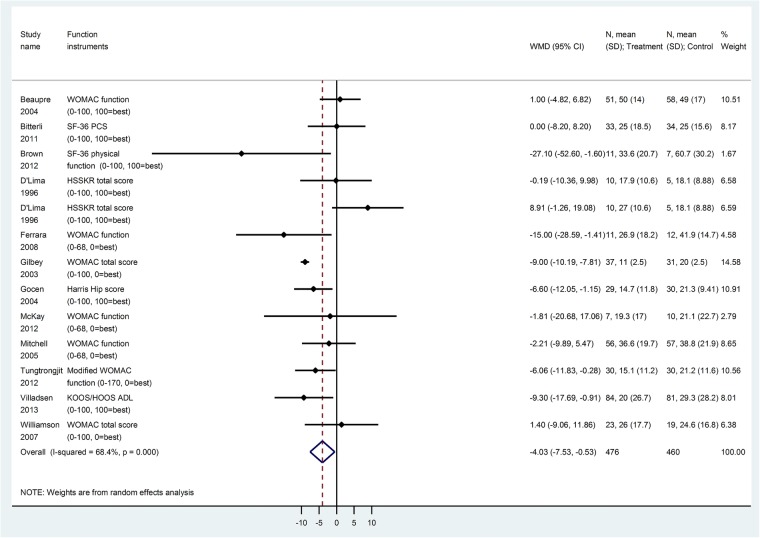
Of 22 studies (1492 patients), 18 had high risk of bias. Prehabilitation slightly reduced pain scores within 4 weeks postoperatively (WMD -6.1 points, 95% CI -10.6 to -1.6 points, on a scale of 0-100), but differences did not remain beyond 4 weeks. Prehabilitation slightly improved WOMAC function score at 6-8 and 12 weeks (WMD -4.0, 95% CI -7.5 to -0.5), and time to climbing stairs (WMD -1.4 days, 95% CI -1.9 to -0.8 days), toilet use (-0.9 days, 95% CI -1.3 to -0.5 days) and chair use (WMD -1.2 days, 95% CI -1.7 to -0.8 days). Effects were similar for knee and hip surgery. Differences were not found for SF-36 scores, length of stay and total cost. Other outcomes of interest were inadequately reported.
Existing evidence suggests that prehabilitation may slightly improve early postoperative pain and function among patients undergoing joint replacement; however, effects remain too small and short-term to be considered clinically-important, and did not affect key outcomes of interest (ie, length of stay, quality of life, costs).
术前物理治疗对关节置换术后恢复的临床影响仍存在争议。本系统评价旨在评估关节置换术前康复的临床影响。
我们检索了截至2015年11月的PubMed、Embase和Cochrane CENTRAL,以查找比较关节置换手术前康复与未进行康复的随机对照试验。术后疼痛和功能评分转换为西安大略和麦克马斯特大学骨关节炎指数(WOMAC)疼痛和功能子量表(0 - 100分,高分表示预后较差)。进行随机效应荟萃分析以计算加权平均差(WMD,95%可信区间),并按髋关节和膝关节手术进行亚组分析。
术后疼痛和功能评分、恢复日常生活活动的时间、生活质量、住院时间、总成本、患者满意度、术后并发症、任何不良事件和停药情况。
在22项研究(1492例患者)中,18项存在高偏倚风险。术前康复在术后4周内使疼痛评分略有降低(WMD -6.1分,95%可信区间 -10.6至 -1.6分,范围为0 - 100分),但4周后差异不再存在。术前康复在6 - 8周和12周时使WOMAC功能评分略有改善(WMD -4.0,95%可信区间 -7.5至 -0.5),以及爬楼梯时间(WMD -1.4天,95%可信区间 -1.9至 -0.8天)、使用厕所时间(-0.9天,95%可信区间 -1.3至 -0.5天)和使用椅子时间(WMD -1.2天,95%可信区间 -1.7至 -0.8天)。膝关节和髋关节手术的效果相似。在SF - 36评分、住院时间和总成本方面未发现差异。其他感兴趣的结局报告不充分。
现有证据表明,术前康复可能会使关节置换患者术后早期疼痛和功能略有改善;然而,效果仍然太小且为短期,不被认为具有临床重要性,并且未影响关键的感兴趣结局(即住院时间、生活质量、成本)。