Verloo Henk, Goulet Céline, Morin Diane, von Gunten Armin
Department Nursing Sciences, University of Applied Sciences, Lausanne, Switzerland.
Faculty of Nursing Science, University of Montreal, Montreal, QC, Canada.
Clin Interv Aging. 2016 Jan 18;11:55-63. doi: 10.2147/CIA.S100576. eCollection 2016.
Delirium and frailty - both potentially reversible geriatric syndromes - are seldom studied together, although they often occur jointly in older patients discharged from hospitals. This study aimed to explore the relationship between delirium and frailty in older adults discharged from hospitals.
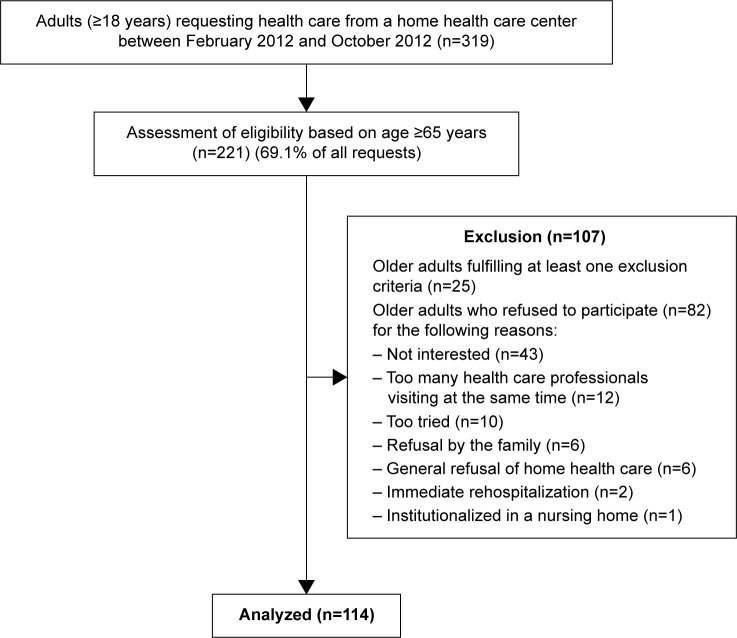
Of the 221 patients aged >65 years, who were invited to participate, only 114 gave their consent to participate in this study. Delirium was assessed using the confusion assessment method, in which patients were classified dichotomously as delirious or nondelirious according to its algorithm. Frailty was assessed using the Edmonton Frailty Scale, which classifies patients dichotomously as frail or nonfrail. In addition to the sociodemographic characteristics, covariates such as scores from the Mini-Mental State Examination, Instrumental Activities of Daily Living scale, and Cumulative Illness Rating Scale for Geriatrics and details regarding polymedication were collected. A multidimensional linear regression model was used for analysis.
Almost 20% of participants had delirium (n=22), and 76.3% were classified as frail (n=87); 31.5% of the variance in the delirium score was explained by frailty (R (2)=0.315). Age; polymedication; scores of the Confusion Assessment Method (CAM), instrumental activities of daily living, and Cumulative Illness Rating Scale for Geriatrics; and frailty increased the predictability of the variance of delirium by 32% to 64% (R (2)=0.64).
Frailty is strongly related to delirium in older patients after discharge from the hospital.
谵妄和衰弱——两种都可能可逆的老年综合征——很少同时进行研究,尽管它们经常共同出现在出院的老年患者中。本研究旨在探讨出院老年患者中谵妄与衰弱之间的关系。
在邀请参与的221名年龄>65岁的患者中,只有114名同意参与本研究。使用混乱评估方法评估谵妄,根据其算法将患者二分法分类为谵妄或非谵妄。使用埃德蒙顿衰弱量表评估衰弱,将患者二分法分类为衰弱或非衰弱。除了社会人口学特征外,还收集了诸如简易精神状态检查表得分、日常生活活动能力量表得分、老年累积疾病评定量表得分以及多重用药的详细信息等协变量。使用多维线性回归模型进行分析。
近20%的参与者患有谵妄(n = 22),76.3%被分类为衰弱(n = 87);衰弱解释了谵妄得分中31.5%的方差(R(2)=0.315)。年龄、多重用药、混乱评估方法(CAM)得分、日常生活活动能力得分、老年累积疾病评定量表得分以及衰弱使谵妄方差的可预测性提高了32%至64%(R(2)=0.64)。
出院后老年患者的衰弱与谵妄密切相关。