Gupta Amita, Montepiedra Grace, Gupte Akshay, Zeldow Bret, Jubulis Jennifer, Detrick Barbara, Violari Avy, Madhi Shabir, Bobat Raziya, Cotton Mark, Mitchell Charles, Spector Stephen
Johns Hopkins University School of Medicine, Baltimore, MD, United States of America.
Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States of America.
PLoS One. 2016 Feb 12;11(2):e0148649. doi: 10.1371/journal.pone.0148649. eCollection 2016.
This study examined the associations of 25-hydroxyvitamin D and specific host genetic variants that affect vitamin D levels or its effects on immune function, with the risk of TB or mortality in children.
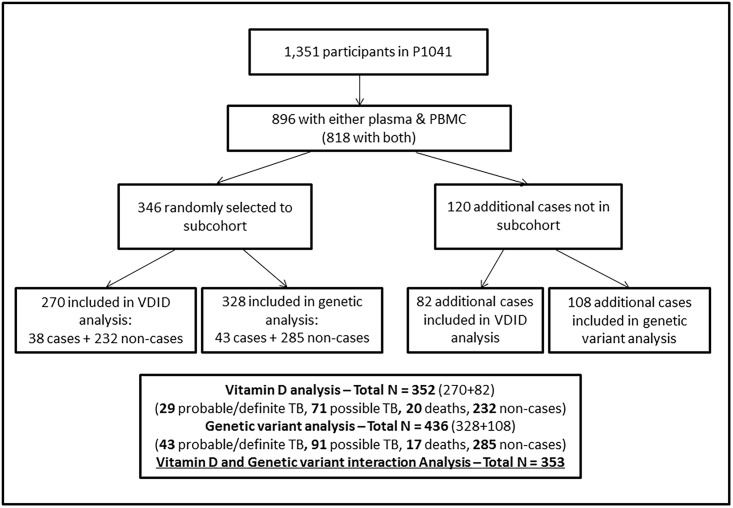
A case-cohort sample of 466 South African infants enrolled in P1041 trial (NCT00080119) underwent 25-hydroxyvitamin D testing by chemiluminescent immunoassay. Single nucleotide polymorphisms (SNPs) that alter the effect of vitamin D [e.g. vitamin D receptor (VDR)], vitamin D levels [e.g. vitamin D binding protein (VDBP)], or toll like receptor (TLR) expression (SIGIRR including adjacent genes PKP3 and TMEM16J) were identified by real-time PCR. Outcomes were time to TB, and to the composite of TB or death by 192 weeks of follow-up. Effect modification between vitamin D status and SNPs for outcomes was assessed.
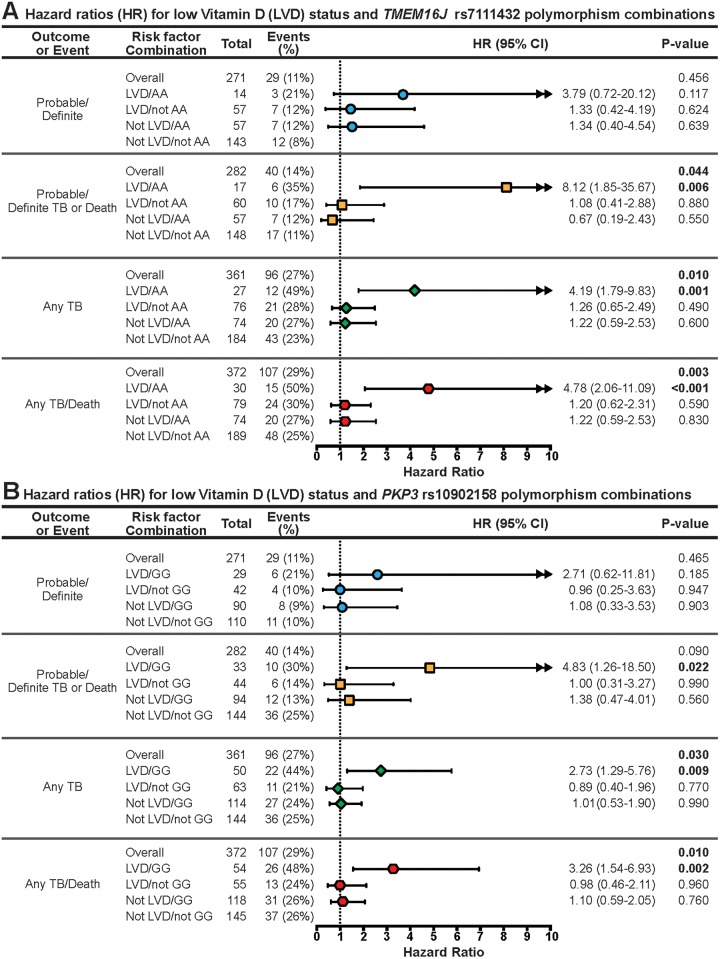
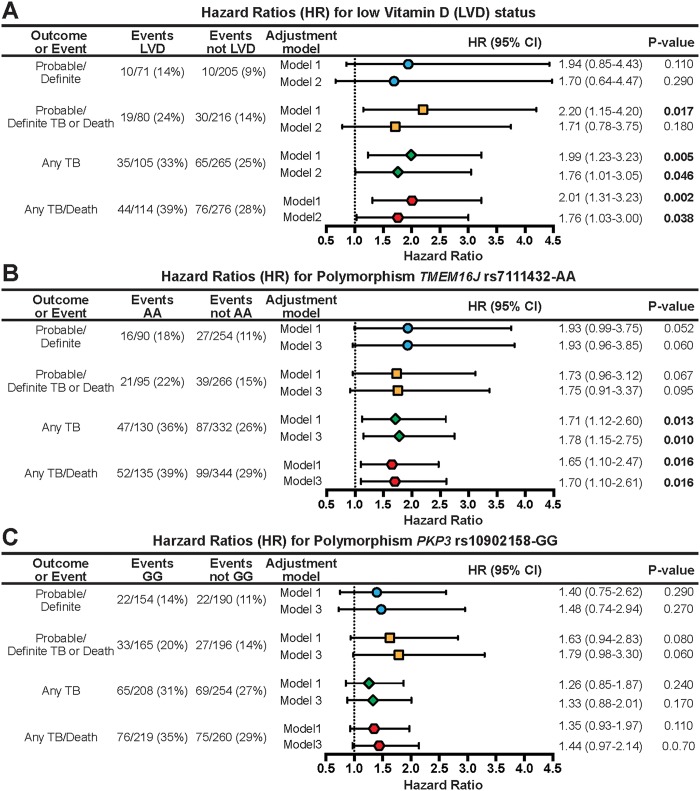
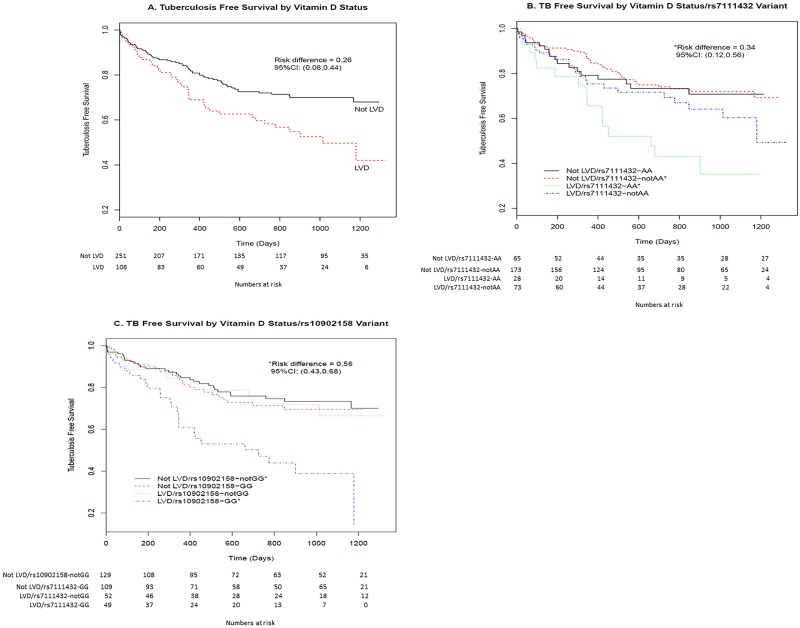
Median age at 25-hydroxyvitamin D determination was 8 months; 11% were breastfed, 51% were HIV-infected and 26% had low 25-hydroxyvitamin D (<32ng/mL). By 192 weeks, 138 incident TB cases (43 definite/probable, and 95 possible) and 26 deaths occurred. Adjusting for HIV status and potential confounders, low 25-hydroxyvitamin D was associated with any TB (adjusted hazard ratio [aHR] 1.76, 95% CI 1.01-3.05; p = 0.046) and any TB or death (aHR 1.76, 95% CI 1.03-3.00; p = 0.038). Children with low 25-hydroxyvitamin D and TMEM 16J rs7111432-AA or PKP3 rs10902158-GG were at increased risk for probable/definite TB or death (aHR 8.12 and 4.83, p<0.05) and any TB or death (aHR 4.78 and 3.26, p<0.005) respectively; SNPs in VDBP, VDR, and vitamin D precursor or hydroxylation genes were not. There was significant interaction between low 25-hydroxyvitamin D and, TMEM 16J rs7111432-AA (p = 0.04) and PKP3 rs10902158-GG (p = 0.02) SNPs.
Two novel SNPs, thought to be associated with innate immunity, in combination with low vitamin D levels were identified as increasing a young child's risk of developing TB disease or death. Identifying high-risk children and providing targeted interventions such as vitamin D supplementation may be beneficial.
ClinicalTrials.gov NCT00080119.
本研究调查了25-羟维生素D以及影响维生素D水平或其免疫功能效应的特定宿主基因变异与儿童结核病风险或死亡率之间的关联。
对参与P1041试验(NCT00080119)的466名南非婴儿的病例队列样本进行化学发光免疫分析以检测25-羟维生素D。通过实时PCR鉴定改变维生素D效应的单核苷酸多态性(SNP)[如维生素D受体(VDR)]、维生素D水平[如维生素D结合蛋白(VDBP)]或Toll样受体(TLR)表达(含相邻基因PKP3和TMEM16J的SIGIRR)。观察指标为结核病发病时间以及随访192周时结核病或死亡的复合终点。评估维生素D状态与SNP对观察指标的效应修饰作用。
测定25-羟维生素D时的中位年龄为8个月;11%为母乳喂养,51%感染艾滋病毒,26%的25-羟维生素D水平较低(<32ng/mL)。到192周时,发生了138例新发结核病病例(43例确诊/疑似,95例可能病例)和26例死亡。校正艾滋病毒状态和潜在混杂因素后,低25-羟维生素D水平与任何类型结核病(校正风险比[aHR]1.76,95%可信区间[CI]1.01 - 3.05;p = 0.046)以及任何类型结核病或死亡(aHR 1.76,95%CI 1.03 - 3.00;p = 0.038)相关。25-羟维生素D水平低且携带TMEM 16J rs7111432-AA或PKP3 rs10902158-GG的儿童发生确诊/疑似结核病或死亡的风险增加(aHR分别为8.12和4.83,p<0.05)以及任何类型结核病或死亡的风险增加(aHR分别为4.78和3.26,p<0.005);VDBP、VDR以及维生素D前体或羟化基因中的SNP则无此关联。低25-羟维生素D水平与TMEM 16J rs7111432-AA(p = 0.04)和PKP3 rs10902158-GG(p = 0.02)的SNP之间存在显著交互作用。
两个被认为与先天免疫相关的新型SNP,与低维生素D水平共同作用,增加了幼儿患结核病或死亡的风险。识别高危儿童并提供针对性干预措施,如补充维生素D,可能有益。
ClinicalTrials.gov NCT00080119。