Hüneburg Robert, Kukuk Guido, Nattermann Jacob, Endler Christoph, Penner Arndt-Hendrik, Wolter Karsten, Schild Hans, Strassburg Christian, Sauerbruch Tilman, Schmitz Volker, Willinek Winfried
Department of Internal Medicine I, University Hospital of Bonn, Bonn, Germany.
Department of Radiology, University Hospital of Bonn, Bonn, Germany.
Endosc Int Open. 2016 Feb;4(2):E164-9. doi: 10.1055/s-0041-111501. Epub 2016 Jan 28.
Colorectal cancer (CRC) is one of the most common cancers worldwide, and several efforts have been made to reduce its occurrence or severity. Although colonoscopy is considered the gold standard in CRC prevention, it has its disadvantages: missed lesions, bleeding, and perforation. Furthermore, a high number of patients undergo this procedure even though no polyps are detected. Therefore, an initial screening examination may be warranted. Our aim was to compare the adenoma detection rate of magnetic resonance colonography (MRC) with that of optical colonoscopy.
A total of 25 patients with an intermediate risk for CRC (17 men, 8 women; mean age 57.6, standard deviation 11) underwent MRC with a 3.0-tesla magnet, followed by colonoscopy. The endoscopist was initially blinded to the results of MRC and unblinded immediately after examining the distal rectum. Following endoscopic excision, the size, anatomical localization, and appearance of all polyps were described according to the Paris classification.
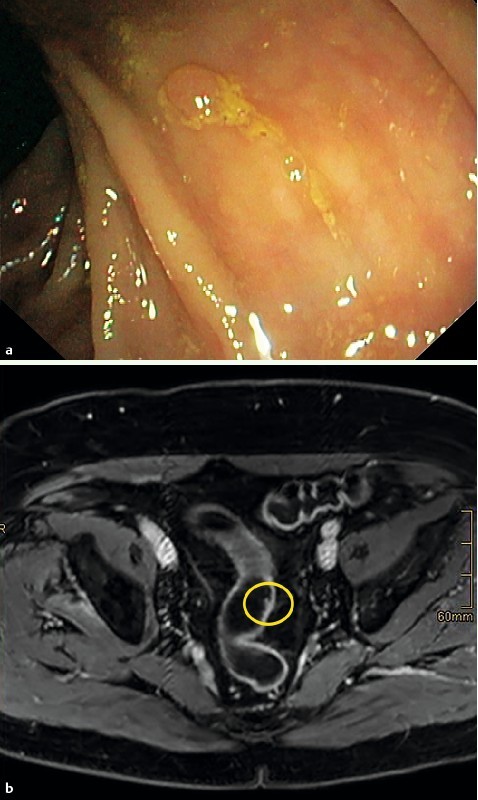
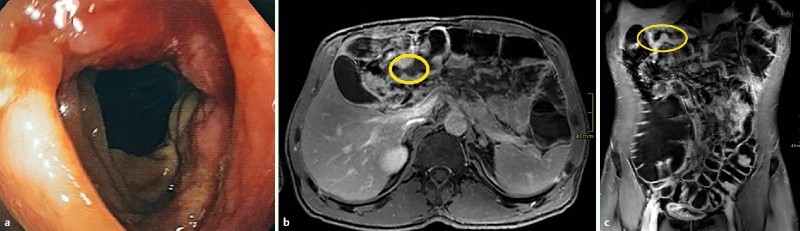
A total of 93 lesions were detected during colonoscopy. These included a malignant infiltration of the transverse colon due to gastric cancer in 1 patient, 28 adenomas in 10 patients, 19 hyperplastic polyps in 9 patients, and 45 non-neoplastic lesions. In 5 patients, no lesion was detected. MRC detected significantly fewer lesions: 1 adenoma (P = 0.001) and 1 hyperplastic polyp (P = 0.004). The malignant infiltration was seen with both modalities. Of the 28 adenomas, 23 (82 %) were 5 mm or smaller; only 4 adenomas 10 mm or larger (14 %) were detected.
MRC does not detect adenomas sufficiently independently of the location of the lesion. Even advanced lesions were missed. Therefore, colonoscopy should still be considered the current gold standard, even for diagnostic purposes.
结直肠癌(CRC)是全球最常见的癌症之一,人们已做出多项努力来降低其发生率或严重程度。尽管结肠镜检查被认为是CRC预防的金标准,但它存在一些缺点:漏诊病变、出血和穿孔。此外,即使未检测到息肉,仍有大量患者接受该检查。因此,可能需要进行初步筛查。我们的目的是比较磁共振结肠成像(MRC)与光学结肠镜检查的腺瘤检出率。
共有25例CRC中度风险患者(17例男性,8例女性;平均年龄57.6岁,标准差11)接受了3.0特斯拉磁共振结肠成像检查,随后进行结肠镜检查。内镜医师最初对MRC结果不知情,在检查直肠远端后立即解除不知情状态。内镜切除后,根据巴黎分类法描述所有息肉的大小、解剖位置和外观。
结肠镜检查共检测到93个病变。其中包括1例因胃癌导致的横结肠恶性浸润、10例患者的28个腺瘤、9例患者的19个增生性息肉和45个非肿瘤性病变。5例患者未检测到病变。MRC检测到的病变明显较少:1个腺瘤(P = 0.001)和1个增生性息肉(P = 0.004)。两种检查方式均发现了恶性浸润。在28个腺瘤中,23个(82%)直径为5毫米或更小;仅检测到4个直径10毫米或更大的腺瘤(14%)。
MRC对腺瘤的检测不够充分,与病变位置无关。即使是晚期病变也会漏诊。因此,即使是出于诊断目的,结肠镜检查仍应被视为当前的金标准。