Baer Alan N, Kurano Tracie, Thakur Uma J, Thawait Gaurav K, Fuld Matthew K, Maynard Janet W, McAdams-DeMarco Mara, Fishman Elliot K, Carrino John A
Department of Medicine (Rheumatology), Johns Hopkins University School of Medicine, 5200 Eastern Avenue, Suite 4000, Mason Lord Center Tower, Baltimore, MD, 21224, USA.
Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
BMC Musculoskelet Disord. 2016 Feb 18;17:91. doi: 10.1186/s12891-016-0943-9.
Dual-energy computed tomography (DECT) is a new diagnostic tool for gout, but its sensitivity has not been established. Our goal was to assess the sensitivity of DECT for the detection of monosodium urate (MSU) deposits in non-tophaceous and tophaceous gout, both at the level of the patient and that of the individual joint or lesion.
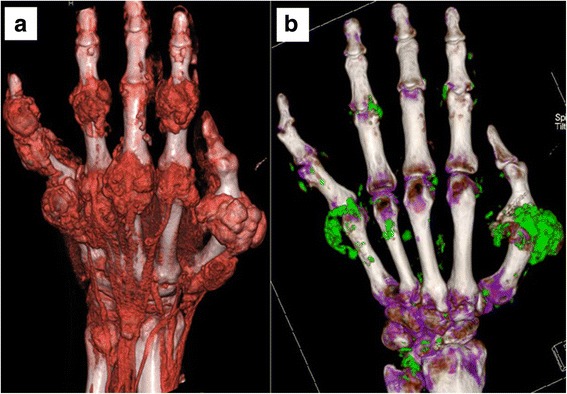
DECT was performed on 11 patients with crystal-proven non-tophaceous gout and 10 with tophaceous gout and included both the upper and lower extremities in 20/21 patients. DECT images were simultaneously acquired at 80 and 140 kV and then processed on a workstation with proprietary software using a two-material decomposition algorithm. MSU deposits were color coded as green by the software and fused onto grey-scale CT images. The number and location of these deposits was tallied independently by two DECT-trained radiologists blinded to the clinical characteristics of the patient. Sensitivity of DECT was defined as the proportion of patients with a confirmed diagnosis of gout which was correctly identified as such by the imaging technique. All patients provided informed consent to participate in this IRB-approved study.
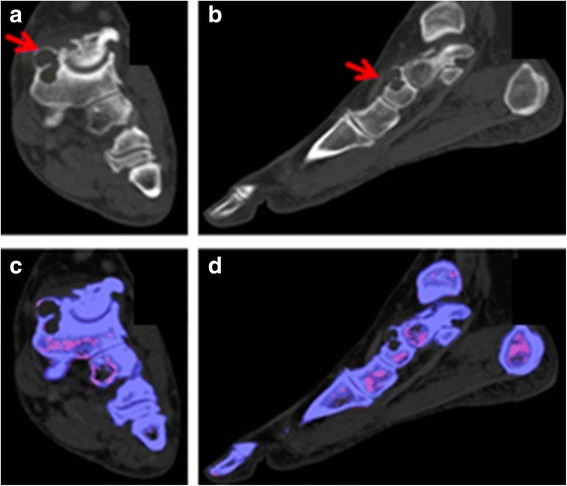
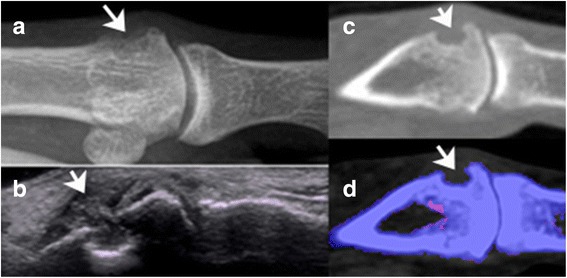
MSU deposits were detected by DECT in ≥1 joint area in 7/11 (64 %) patients with non-tophaceous gout, but were only detected in 3/12 (25 %) joints proven by aspiration to be affected with gout. Inclusion of the upper extremity joints in the scanning protocol did not improve sensitivity. All 10 patients with tophaceous gout had MSU deposits evident by DECT. The sensitivity of DECT for individual gouty erosions was assessed in 3 patients with extensive foot involvement. MSU deposits were detected by DECT within or immediately adjacent to 13/26 (50 %) erosions.
A DECT protocol that includes all lower extremity joints has moderate sensitivity in non-tophaceous and high sensitivity in tophaceous gout. However, DECT has lower sensitivity when restricted to individual crystal-proven gouty joints in non-tophaceous disease or individual erosive lesions in tophaceous gout. The detection of MSU deposits by DECT relates to their size and density and the detection parameters of the DECT scanner and adjustment of the latter might improve sensitivity.
双能计算机断层扫描(DECT)是一种用于痛风的新型诊断工具,但其敏感性尚未确定。我们的目标是评估DECT在检测非痛风石性和痛风石性痛风患者中尿酸钠(MSU)沉积的敏感性,包括患者层面以及个体关节或病变层面。
对11例经晶体证实的非痛风石性痛风患者和10例痛风石性痛风患者进行了DECT检查,20/21例患者的上下肢均纳入检查范围。在80 kV和140 kV同时采集DECT图像,然后在工作站上使用专有软件通过双物质分解算法进行处理。软件将MSU沉积物编码为绿色,并融合到灰度CT图像上。两名接受过DECT培训的放射科医生在不知道患者临床特征的情况下,独立统计这些沉积物的数量和位置。DECT的敏感性定义为经影像学技术正确识别出确诊痛风患者的比例。所有患者均签署知情同意书,参与这项经机构审查委员会批准的研究。
在7/11(64%)例非痛风石性痛风患者中,DECT在≥1个关节区域检测到MSU沉积,但在经抽吸证实受痛风影响的3/12(25%)个关节中仅检测到MSU沉积。扫描方案中纳入上肢关节并未提高敏感性。所有10例痛风石性痛风患者的MSU沉积在DECT上均明显可见。对3例足部广泛受累的患者评估了DECT对单个痛风性侵蚀的敏感性。在13/26(50%)个侵蚀部位内或紧邻部位,DECT检测到了MSU沉积。
包括所有下肢关节的DECT方案在非痛风石性痛风中具有中等敏感性,在痛风石性痛风中具有高敏感性。然而,在非痛风石性疾病中,当仅限于经晶体证实的单个痛风性关节或痛风石性痛风中的单个侵蚀性病变时,DECT的敏感性较低。DECT对MSU沉积的检测与其大小和密度有关,调整DECT扫描仪的检测参数可能会提高敏感性。