Leone Antonio Maria, D'Amario Domenico, Teofili Luciana, Basile Eloisa, Cannata Francesco, Graziani Francesca, Marzilli Mario, Russo Antonio Matteo, Tarantini Giuseppe, Ceconi Claudio, Leone Giuseppe, Trani Carlo, Rebuzzi Antonio Giuseppe, Crea Filippo
Dipartimento di Scienze Cardiovascolari, Università Cattolica del Sacro Cuore, Largo Agostino Gemelli, 8, Rome, 00168, Italy.
Istituto di Ematologia, Università Cattolica del Sacro Cuore, Largo Agostino Gemelli, 8, Rome, 00168, Italy.
Trials. 2016 Feb 19;17:97. doi: 10.1186/s13063-016-1172-0.
Several clinical trials and recent meta-analyses have demonstrated that administration of recombinant human granulocyte-colony stimulating factor (G-CSF) is safe and, only in patients with large acute myocardial infarction (AMI), is associated with an improvement in left ventricular ejection fraction. Moreover, the mobilization and engraftment of the bone marrow-derived cells may differ significantly among patients, interfering with the restoration of left ventricular function after treatment. Therefore, the clinical potential application of the G-CSF has not yet been fully elucidated.
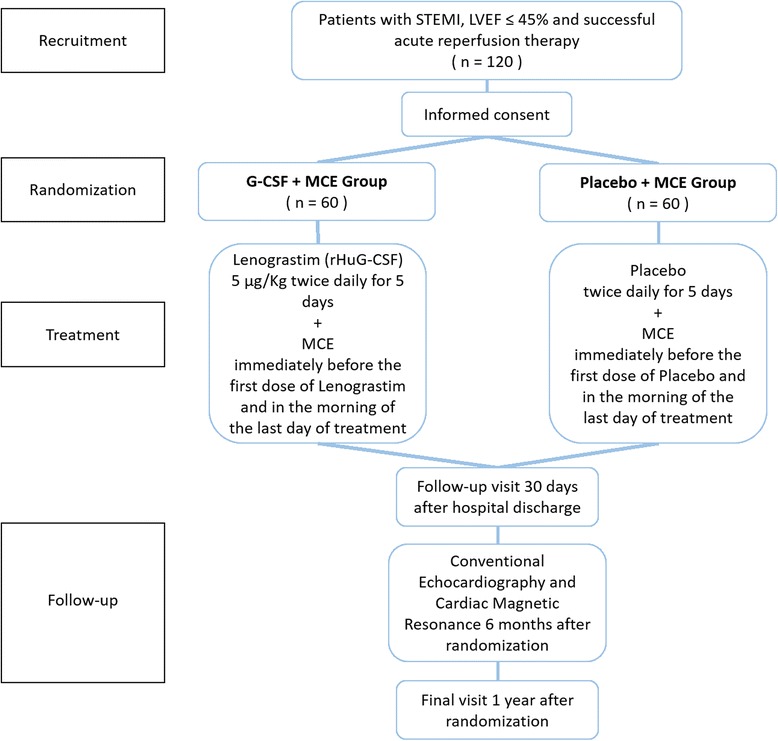
METHODS/DESIGN: The RIGENERA 2.0 trial is a multicenter, phase II, placebo-controlled, randomized, open-label, with blinded evaluation of endpoints (PROBE) trial in which 120 patients with an acute ST-elevation myocardial infarction (STEMI) undergoing successful revascularization but with residual myocardial dysfunction will be enrolled. In cases where there is a left ventricular ejection fraction (LVEF) ≤ 45% the patient will be electronically randomized (1:1 ratio) to receive either subcutaneous recombinant human G-CSF (group 1) or placebo (group 2) both added on top of optimal standard of care. Both groups will undergo myocardial contrast echocardiography with intravenous infusion of sulfur hexafluoride (MCE) whilst undergoing the echocardiogram. The primary efficacy endpoint is the evaluation of the LVEF at 6 months after AMI assessed by cardiac magnetic resonance. Secondary efficacy endpoints are the evaluation of LVEF at 6 months after AMI assessed by echocardiography, left ventricular end-diastolic volume (LVEDV) and left ventricular end-systolic volume (LVESV) assessed by cardiac magnetic resonance and echocardiography at 6 months, together with the incidence of major adverse clinical events (MACE) defined as death, myocardial infarction, sustained cardiac arrhythmias, cardiogenic shock, stroke and re-hospitalization due to heart failure at 1 year.
The RIGENERA 2.0 trial will test whether G-CSF administration and MCE, through the enhancement of the bone marrow-derived cells homing in the myocardium, determines an improvement in regional and global contractile function, myocardial perfusion and infarct extension in patients with large AMI. The results of the present study are expected to envision routine clinical use of this safe, affordable and reproducible approach in patients with successful revascularization after AMI.
ClinicalTrials.gov: NCT02502747 (29 June 2015); EudraCT: 2015-002189-21 (10 July 2015).
多项临床试验及近期的荟萃分析表明,给予重组人粒细胞集落刺激因子(G-CSF)是安全的,且仅在大面积急性心肌梗死(AMI)患者中,其与左心室射血分数的改善相关。此外,骨髓来源细胞的动员和植入在患者之间可能存在显著差异,这会干扰治疗后左心室功能的恢复。因此,G-CSF的临床潜在应用尚未完全阐明。
方法/设计:RIGENERA 2.0试验是一项多中心、II期、安慰剂对照、随机、开放标签、终点盲法评估(PROBE)试验,将纳入120例急性ST段抬高型心肌梗死(STEMI)且成功进行血运重建但仍存在残余心肌功能障碍的患者。若左心室射血分数(LVEF)≤45%,患者将通过电子随机分组(1:1比例),接受皮下注射重组人G-CSF(第1组)或安慰剂(第2组),二者均在最佳标准治疗基础上使用。两组在进行超声心动图检查时,均将接受静脉注射六氟化硫的心肌对比超声心动图检查(MCE)。主要疗效终点是通过心脏磁共振评估AMI后6个月时的LVEF。次要疗效终点包括通过超声心动图评估AMI后6个月时的LVEF、通过心脏磁共振和超声心动图评估6个月时的左心室舒张末期容积(LVEDV)和左心室收缩末期容积(LVESV),以及定义为1年内死亡、心肌梗死、持续性心律失常、心源性休克、中风和因心力衰竭再次住院的主要不良临床事件(MACE)的发生率。
RIGENERA 2.0试验将测试给予G-CSF和MCE是否通过增强骨髓来源细胞归巢至心肌,从而改善大面积AMI患者的局部和整体收缩功能、心肌灌注及梗死范围。本研究结果有望为AMI后成功进行血运重建的患者设想这种安全、经济且可重复的方法在常规临床中的应用。
ClinicalTrials.gov:NCT02502747(2015年6月29日);EudraCT:2015-002189-21(2015年7月10日)。