Dy Geolani W, Hsi Ryan S, Holt Sarah K, Lendvay Thomas S, Gore John L, Harper Jonathan D
Department of Urology, University of Washington School of Medicine, Seattle, Washington.
Department of Urology, University of Washington School of Medicine, Seattle, Washington.
J Urol. 2016 Apr;195(4 Pt 2):1209-14. doi: 10.1016/j.juro.2015.11.010. Epub 2016 Feb 28.
Although reported success rates after pediatric pyeloplasty to correct ureteropelvic junction are high, failure may require intervention. We sought to characterize the incidence and timing of secondary procedures after pediatric pyeloplasty using a national employer based insurance database.
Using the MarketScan® database we identified patients 0 to 18 years old who underwent pyeloplasty from 2007 to 2013 with greater than 3 months of postoperative enrollment. Secondary procedures following the index pyeloplasty were identified by CPT codes and classified as stent/drain, endoscopic, pyeloplasty, nephrectomy or transplant. The risk of undergoing a secondary procedure was ascertained using Cox proportional hazards models adjusting for demographic and clinical characteristics.
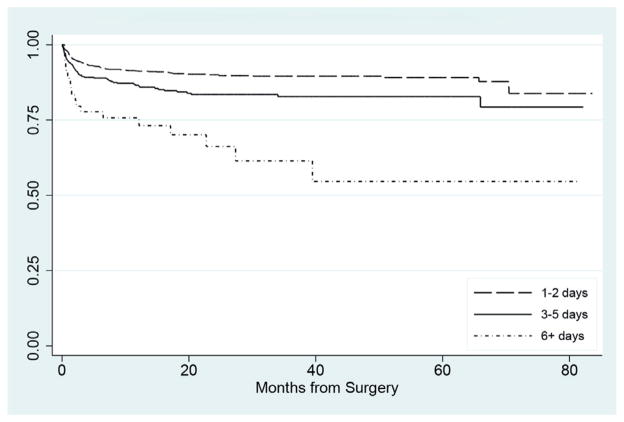
We identified 1,976 patients with a mean ± SD followup of 23.9 ± 19.8 months. Overall 226 children (11.4%) had undergone at least 1 post-pyeloplasty procedure. The first procedure was done within 1 year in 87.2% of patients with a mean postoperative interval of 5.9 ± 11.1 months. Stents/drains, endoscopic procedures and pyeloplasties were noted in 116 (5.9%), 34 (1.7%) and 71 patients (3.1%), respectively. Length of stay was associated with undergoing a secondary procedure. Compared with 2 days or less the HR of 3 to 5 and 6 days or greater was 1.65 and 3.94 (p = 0.001 and <0.001, respectively).
Following pediatric pyeloplasty 1 of 9 patients undergoes at least 1 secondary procedure with the majority performed within the first year. One of 11 patients undergoes intervention more extensive than placement of a single stent or drain, requiring management strategies that generally signify recurrent or persistent obstruction. Estimates of pyeloplasty success in this national data set are lower than in other published series.
尽管据报道小儿肾盂成形术矫正肾盂输尿管连接部的成功率很高,但失败时可能需要进一步干预。我们试图利用一个全国性的雇主医保数据库来描述小儿肾盂成形术后二次手术的发生率及时间。
利用MarketScan®数据库,我们确定了2007年至2013年接受肾盂成形术且术后登记时间超过3个月的0至18岁患者。初次肾盂成形术后的二次手术通过现行程序编码(CPT)识别,并分类为支架/引流管、内镜、肾盂成形术、肾切除术或移植术。采用Cox比例风险模型确定二次手术风险,并对人口统计学和临床特征进行校正。
我们确定了1976例患者,平均随访时间为23.9±19.8个月。总体而言,226名儿童(11.4%)至少接受了1次肾盂成形术后手术。87.2%的患者在1年内进行了首次手术,术后平均间隔时间为5.9±11.1个月。分别有116例(5.9%)、34例(1.7%)和71例患者(3.1%)进行了支架/引流管、内镜手术和肾盂成形术。住院时间与二次手术有关。与住院2天或更短时间相比,住院3至5天和6天或更长时间的风险比分别为1.65和3.94(p分别为0.001和<0.001)。
小儿肾盂成形术后,9名患者中有1名至少接受1次二次手术,大多数在第一年内进行。11名患者中有1名接受的干预比单纯放置支架或引流管更为广泛,这需要一些管理策略,这些策略通常意味着复发或持续性梗阻。该全国性数据集中肾盂成形术的成功率估计低于其他已发表系列。