Yue Yong, Astvatsaturyan Kristine, Cui Xiaojiang, Zhang Xiao, Fraass Benedick, Bose Shikha
Department of Radiation Oncology, Cedars-Sinai Medical Center, Los Angeles, California, United States of America.
Department of Pathology, Cedars-Sinai Medical Center, Los Angeles, California, United States of America.
PLoS One. 2016 Mar 1;11(3):e0149661. doi: 10.1371/journal.pone.0149661. eCollection 2016.
Triple-negative breast cancer (TNBC) is highly diverse group of cancers, and generally considered an aggressive disease associated with poor survival. Stratification of TNBC is highly desired for both prognosis and treatment decisions to identify patients who may benefit from less aggressive therapy.
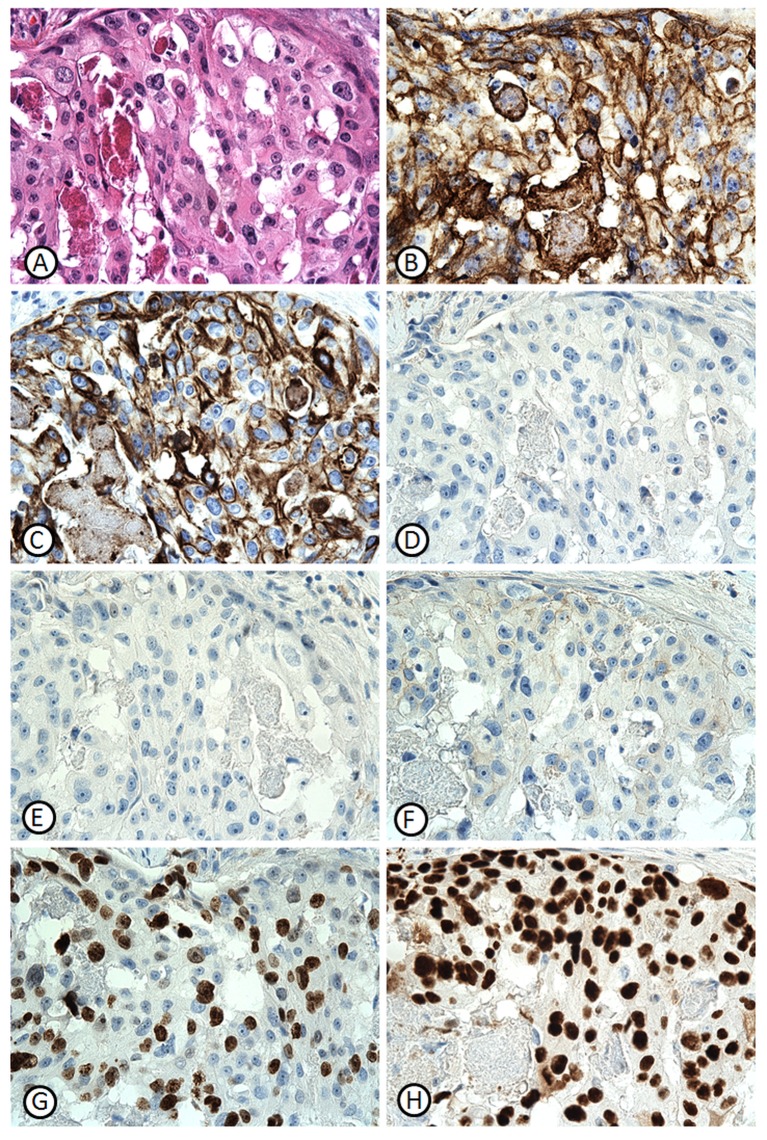
This study retrieved 192 consecutive non-metastasis TNBC patients who had undergone a resection of a primary tumor from 2008 to 2012. All samples were negative for ER, PR, and HER2/neu. Disease-free-survival (DFS) and overall-survival (OS) were evaluated for expression of immunohistochemical biomarkers (P53, Ki-67, CK5/6 and EGFR), as well as clinicopathological variables including age, tumor size, grade, lymph node status, pathologic tumor and nodal stages. The cutoff values of the basal biomarkers, EGFR and CK5/6, were estimated by time-dependent ROC curves. The prognostic values of combinatorial variables were identified by univariate and multivariate Cox analysis. Patients were stratified into different risk groups based on expression status of identified prognostic variables.
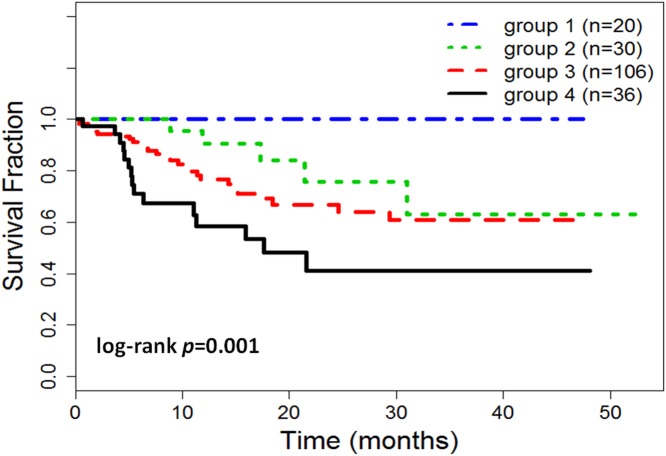
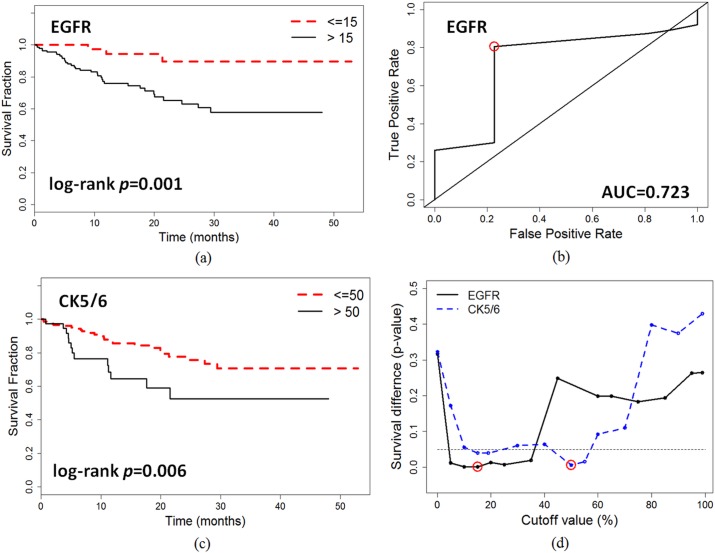
Median age was 57 years (range, 28-92 years). Patients' tumor stage and nodal stage were significantly associated with OS and DFS. EGFR and CK5/6 were significant prognostic variables at cutoff points of 15% (p = 0.001, AUC = 0.723), and 50% (p = 0.006, AUC = 0.675), respectively. Multivariate Cox analysis identified five significant variables: EGFR (p = 0.016), CK5/6 (p = 0.018), Ki-67 (p = 0.048), tumor stage (p = 0.010), and nodal stage (p = 0.003). Patients were stratified into low basal (EGFR≤15% and CK5/6≤50%) and high basal (EGFR>15% and/or CK5/6>50%) expression groups. In the low basal expression group, patients with low expressions of Ki-67, low tumor and nodal stage had significantly better survival than those with high expressions/stages of three variables, log-rank p = 0.015 (100% vs 68% at 50 months). In the high basal expression group, patient with high basal expression of both biomarkers (EGFR >15% and CK5/6 >50%) had worse survival (mean DFS = 25 months, 41.7% event rate) than those patient with high expression of either one marker (mean DFS = 34 months, 25.5% event rate).
Immunoexpression of basal biomarkers, EGFR and CK5/6, is useful in predicting survival of TNBC patients. Integrated with Ki-67, tumor and nodal stages, combinatorial biomarker analysis provides a feasible clinical solution to stratify patient risks and help clinical decision-making with respect to selecting the appropriate therapies for individual patients.
三阴性乳腺癌(TNBC)是一组高度异质性的癌症,通常被认为是一种侵袭性疾病,预后较差。为了进行预后评估和治疗决策,以确定可能从较温和治疗中获益的患者,对TNBC进行分层非常必要。
本研究纳入了2008年至2012年期间连续192例接受原发性肿瘤切除术的非转移性TNBC患者。所有样本的雌激素受体(ER)、孕激素受体(PR)和人表皮生长因子受体2(HER2/neu)均为阴性。通过免疫组化生物标志物(P53、Ki-67、细胞角蛋白5/6(CK5/6)和表皮生长因子受体(EGFR))的表达情况以及包括年龄、肿瘤大小、分级、淋巴结状态、病理肿瘤分期和淋巴结分期等临床病理变量来评估无病生存期(DFS)和总生存期(OS)。通过时间依赖性ROC曲线估计基础生物标志物EGFR和CK5/6的临界值。通过单因素和多因素Cox分析确定组合变量的预后价值。根据已确定的预后变量的表达状态将患者分为不同的风险组。
中位年龄为57岁(范围28 - 92岁)。患者的肿瘤分期和淋巴结分期与OS和DFS显著相关。EGFR和CK5/6在临界值分别为15%(p = 0.001,曲线下面积(AUC) = 0.723)和50%(p = 0.006,AUC = 0.675)时是显著的预后变量。多因素Cox分析确定了五个显著变量:EGFR(p = 0.016)、CK5/6(p = 0.018)、Ki-67(p = 0.048)、肿瘤分期(p = 0.010)和淋巴结分期(p = 0.003)。患者被分为低基础表达组(EGFR≤15%且CK5/6≤50%)和高基础表达组(EGFR>15%和/或CK5/6>50%)。在低基础表达组中,Ki-67低表达、肿瘤和淋巴结分期低的患者的生存期明显优于这三个变量高表达/高分期的患者,对数秩检验p = 0.015(50个月时为100%对68%)。在高基础表达组中,两种生物标志物基础表达均高(EGFR >15%且CK5/6 >50%)的患者的生存期(平均DFS = 25个月,事件发生率41.7%)比仅一种标志物高表达的患者(平均DFS = 34个月,事件发生率25.5%)更差。
基础生物标志物EGFR和CK5/6的免疫表达有助于预测TNBC患者的生存期。结合Ki-67、肿瘤和淋巴结分期,组合生物标志物分析为分层患者风险提供了一种可行的临床解决方案,并有助于临床决策,为个体患者选择合适的治疗方法。