Sissoko Daouda, Laouenan Cedric, Folkesson Elin, M'Lebing Abdoul-Bing, Beavogui Abdoul-Habib, Baize Sylvain, Camara Alseny-Modet, Maes Piet, Shepherd Susan, Danel Christine, Carazo Sara, Conde Mamoudou N, Gala Jean-Luc, Colin Géraldine, Savini Hélène, Bore Joseph Akoi, Le Marcis Frederic, Koundouno Fara Raymond, Petitjean Frédéric, Lamah Marie-Claire, Diederich Sandra, Tounkara Alexis, Poelart Geertrui, Berbain Emmanuel, Dindart Jean-Michel, Duraffour Sophie, Lefevre Annabelle, Leno Tamba, Peyrouset Olivier, Irenge Léonid, Bangoura N'Famara, Palich Romain, Hinzmann Julia, Kraus Annette, Barry Thierno Sadou, Berette Sakoba, Bongono André, Camara Mohamed Seto, Chanfreau Munoz Valérie, Doumbouya Lanciné, Kighoma Patient Mumbere, Koundouno Fara Roger, Loua Cécé Moriba, Massala Vincent, Moumouni Kinda, Provost Célia, Samake Nenefing, Sekou Conde, Soumah Abdoulaye, Arnould Isabelle, Komano Michel Saa, Gustin Lina, Berutto Carlotta, Camara Diarra, Camara Fodé Saydou, Colpaert Joliene, Delamou Léontine, Jansson Lena, Kourouma Etienne, Loua Maurice, Malme Kristian, Manfrin Emma, Maomou André, Milinouno Adele, Ombelet Sien, Sidiboun Aboubacar Youla, Verreckt Isabelle, Yombouno Pauline, Bocquin Anne, Carbonnelle Caroline, Carmoi Thierry, Frange Pierre, Mely Stéphane, Nguyen Vinh-Kim, Pannetier Delphine, Taburet Anne-Marie, Treluyer Jean-Marc, Kolie Jacques, Moh Raoul, Gonzalez Minerva Cervantes, Kuisma Eeva, Liedigk Britta, Ngabo Didier, Rudolf Martin, Thom Ruth, Kerber Romy, Gabriel Martin, Di Caro Antonino, Wölfel Roman, Badir Jamal, Bentahir Mostafa, Deccache Yann, Dumont Catherine, Durant Jean-François, El Bakkouri Karim, Gasasira Uwamahoro Marie, Smits Benjamin, Toufik Nora, Van Cauwenberghe Stéphane, Ezzedine Khaled, D'Ortenzio Eric, Pizarro Louis, Etienne Aurélie, Guedj Jérémie, Fizet Alexandra, Barte de Sainte Fare Eric, Murgue Bernadette, Tran-Minh Tuan, Rapp Christophe, Piguet Pascal, Poncin Marc, Draguez Bertrand, Allaford Duverger Thierry, Barbe Solenne, Baret Guillaume, Defourny Isabelle, Carroll Miles, Raoul Hervé, Augier Augustin, Eholie Serge P, Yazdanpanah Yazdan, Levy-Marchal Claire, Antierrens Annick, Van Herp Michel, Günther Stephan, de Lamballerie Xavier, Keïta Sakoba, Mentre France, Anglaret Xavier, Malvy Denis
Inserm, UMR 1219, Université de Bordeaux, Bordeaux, France.
Centre Hospitalier Universitaire de Bordeaux, Bordeaux, France.
PLoS Med. 2016 Mar 1;13(3):e1001967. doi: 10.1371/journal.pmed.1001967. eCollection 2016 Mar.
Ebola virus disease (EVD) is a highly lethal condition for which no specific treatment has proven efficacy. In September 2014, while the Ebola outbreak was at its peak, the World Health Organization released a short list of drugs suitable for EVD research. Favipiravir, an antiviral developed for the treatment of severe influenza, was one of these. In late 2014, the conditions for starting a randomized Ebola trial were not fulfilled for two reasons. One was the perception that, given the high number of patients presenting simultaneously and the very high mortality rate of the disease, it was ethically unacceptable to allocate patients from within the same family or village to receive or not receive an experimental drug, using a randomization process impossible to understand by very sick patients. The other was that, in the context of rumors and distrust of Ebola treatment centers, using a randomized design at the outset might lead even more patients to refuse to seek care. Therefore, we chose to conduct a multicenter non-randomized trial, in which all patients would receive favipiravir along with standardized care. The objectives of the trial were to test the feasibility and acceptability of an emergency trial in the context of a large Ebola outbreak, and to collect data on the safety and effectiveness of favipiravir in reducing mortality and viral load in patients with EVD. The trial was not aimed at directly informing future guidelines on Ebola treatment but at quickly gathering standardized preliminary data to optimize the design of future studies.
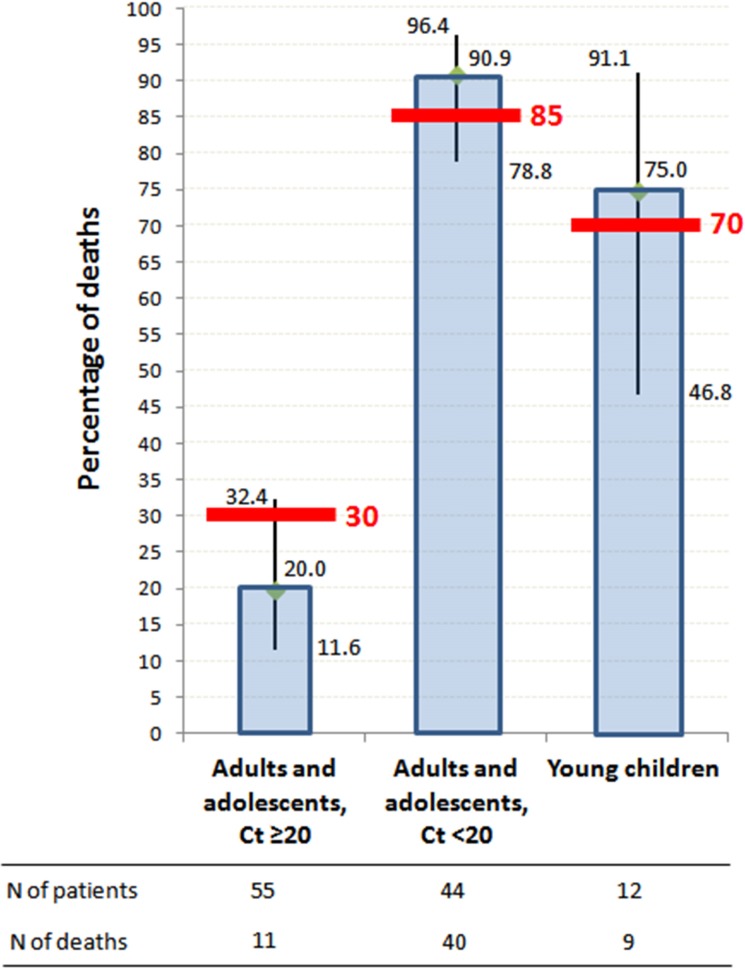
Inclusion criteria were positive Ebola virus reverse transcription PCR (RT-PCR) test, age ≥ 1 y, weight ≥ 10 kg, ability to take oral drugs, and informed consent. All participants received oral favipiravir (day 0: 6,000 mg; day 1 to day 9: 2,400 mg/d). Semi-quantitative Ebola virus RT-PCR (results expressed in "cycle threshold" [Ct]) and biochemistry tests were performed at day 0, day 2, day 4, end of symptoms, day 14, and day 30. Frozen samples were shipped to a reference biosafety level 4 laboratory for RNA viral load measurement using a quantitative reference technique (genome copies/milliliter). Outcomes were mortality, viral load evolution, and adverse events. The analysis was stratified by age and Ct value. A "target value" of mortality was defined a priori for each stratum, to guide the interpretation of interim and final analysis. Between 17 December 2014 and 8 April 2015, 126 patients were included, of whom 111 were analyzed (adults and adolescents, ≥13 y, n = 99; young children, ≤6 y, n = 12). Here we present the results obtained in the 99 adults and adolescents. Of these, 55 had a baseline Ct value ≥ 20 (Group A Ct ≥ 20), and 44 had a baseline Ct value < 20 (Group A Ct < 20). Ct values and RNA viral loads were well correlated, with Ct = 20 corresponding to RNA viral load = 7.7 log10 genome copies/ml. Mortality was 20% (95% CI 11.6%-32.4%) in Group A Ct ≥ 20 and 91% (95% CI 78.8%-91.1%) in Group A Ct < 20. Both mortality 95% CIs included the predefined target value (30% and 85%, respectively). Baseline serum creatinine was ≥110 μmol/l in 48% of patients in Group A Ct ≥ 20 (≥300 μmol/l in 14%) and in 90% of patients in Group A Ct < 20 (≥300 μmol/l in 44%). In Group A Ct ≥ 20, 17% of patients with baseline creatinine ≥110 μmol/l died, versus 97% in Group A Ct < 20. In patients who survived, the mean decrease in viral load was 0.33 log10 copies/ml per day of follow-up. RNA viral load values and mortality were not significantly different between adults starting favipiravir within <72 h of symptoms compared to others. Favipiravir was well tolerated.
In the context of an outbreak at its peak, with crowded care centers, randomizing patients to receive either standard care or standard care plus an experimental drug was not felt to be appropriate. We did a non-randomized trial. This trial reaches nuanced conclusions. On the one hand, we do not conclude on the efficacy of the drug, and our conclusions on tolerance, although encouraging, are not as firm as they could have been if we had used randomization. On the other hand, we learned about how to quickly set up and run an Ebola trial, in close relationship with the community and non-governmental organizations; we integrated research into care so that it improved care; and we generated knowledge on EVD that is useful to further research. Our data illustrate the frequency of renal dysfunction and the powerful prognostic value of low Ct values. They suggest that drug trials in EVD should systematically stratify analyses by baseline Ct value, as a surrogate of viral load. They also suggest that favipiravir monotherapy merits further study in patients with medium to high viremia, but not in those with very high viremia.
ClinicalTrials.gov NCT02329054.
埃博拉病毒病(EVD)是一种致死率很高的疾病,尚无经证实有效的特异性治疗方法。2014年9月,在埃博拉疫情达到高峰时,世界卫生组织公布了一份适合埃博拉病毒病研究的药物简短清单。法匹拉韦是一种用于治疗严重流感的抗病毒药物,是其中之一。2014年末,启动埃博拉随机试验的条件因两个原因未能满足。其一,鉴于同时出现症状的患者数量众多且该疾病死亡率极高,采用一种病情严重的患者无法理解的随机化程序,将来自同一家族或村庄的患者分配接受或不接受试验药物,在伦理上是不可接受的。其二,在存在对埃博拉治疗中心的谣言和不信任的背景下,从一开始就采用随机设计可能会导致更多患者拒绝寻求治疗。因此,我们选择进行一项多中心非随机试验,所有患者都将接受法匹拉韦以及标准化治疗。该试验的目的是检验在大规模埃博拉疫情背景下进行紧急试验的可行性和可接受性,并收集关于法匹拉韦在降低埃博拉病毒病患者死亡率和病毒载量方面的安全性和有效性的数据。该试验并非旨在直接为未来的埃博拉治疗指南提供依据,而是旨在快速收集标准化的初步数据以优化未来研究的设计。
纳入标准为埃博拉病毒逆转录聚合酶链反应(RT-PCR)检测呈阳性、年龄≥1岁、体重≥10千克、能够口服药物且签署知情同意书。所有参与者均口服法匹拉韦(第0天:6000毫克;第1天至第9天:2400毫克/天)。在第0天、第2天、第4天、症状结束时、第14天和第30天进行半定量埃博拉病毒RT-PCR(结果以“循环阈值”[Ct]表示)和生化检测。将冷冻样本运送至一个参考生物安全4级实验室,采用定量参考技术(基因组拷贝数/毫升)测量RNA病毒载量。观察指标为死亡率、病毒载量变化及不良事件。分析按年龄和Ct值分层。为指导中期和最终分析,为每个分层预先定义了一个死亡率“目标值”。在2014年12月17日至2015年4月8日期间,共纳入126例患者,其中111例进行了分析(成人和青少年,≥13岁,n = 99;幼儿,≤6岁,n = 12)。在此我们展示在99例成人和青少年中获得的结果。其中,55例基线Ct值≥20(A组Ct≥20),44例基线Ct值<20(A组Ct<20)。Ct值与RNA病毒载量高度相关,Ct = 20对应RNA病毒载量 = 7.7 log10基因组拷贝/毫升。A组Ct≥20的死亡率为20%(95%CI 11.6% - 32.4%),A组Ct<20的死亡率为91%(95%CI 78.8% - 91.1%)。两个死亡率的95%CI均包含预先定义的目标值(分别为30%和85%)。A组Ct≥20的患者中48%基线血清肌酐≥110μmol/L(14%≥300μmol/L),A组Ct<20的患者中90%基线血清肌酐≥110μmol/L(44%≥300μmol/L)。在A组Ct≥20中,基线肌酐≥110μmol/L的患者中有17%死亡,而在A组Ct<20中这一比例为97%。在存活患者中,随访期间病毒载量平均每天下降0.33 log10拷贝/毫升。与其他患者相比,在症状出现<72小时内开始使用法匹拉韦的成人患者的RNA病毒载量值和死亡率无显著差异。法匹拉韦耐受性良好。
在疫情高峰期且医疗中心拥挤的情况下,将患者随机分配接受标准治疗或标准治疗加试验药物被认为是不合适的。我们进行了一项非随机试验。该试验得出了细微差别明显的结论。一方面,我们未得出关于该药物疗效的结论,并且我们关于耐受性的结论尽管令人鼓舞,但如果采用随机化,可能不会如此确凿。另一方面,我们了解了如何与社区和非政府组织密切合作快速建立并开展一项埃博拉试验;我们将研究融入治疗从而改善了治疗;并且我们生成了对进一步研究有用的关于埃博拉病毒病的知识。我们的数据说明了肾功能不全的发生率以及低Ct值强大的预后价值。它们表明埃博拉病毒病药物试验应系统地按基线Ct值分层分析,作为病毒载量的替代指标。它们还表明,法匹拉韦单药治疗对于中高病毒血症患者值得进一步研究,但对于病毒血症极高的患者则不然。
ClinicalTrials.gov NCT02329054