Kenyon Sara, Jolly Kate, Hemming Karla, Hope Lucy, Blissett Jackie, Dann Sophie-Anna, Lilford Richard, MacArthur Christine
Institute of Applied Health Research, College of Medical and Dental Sciences University of Birmingham, Birmingham, UK.
University of Worcester.
BMJ Open. 2016 Mar 2;6(3):e009203. doi: 10.1136/bmjopen-2015-009203.
We sought evidence of effectiveness of lay support to improve maternal and child outcomes in disadvantaged families.
Prospective, pragmatic, individually randomised controlled trial.
3 Maternity Trusts in West Midlands, UK.
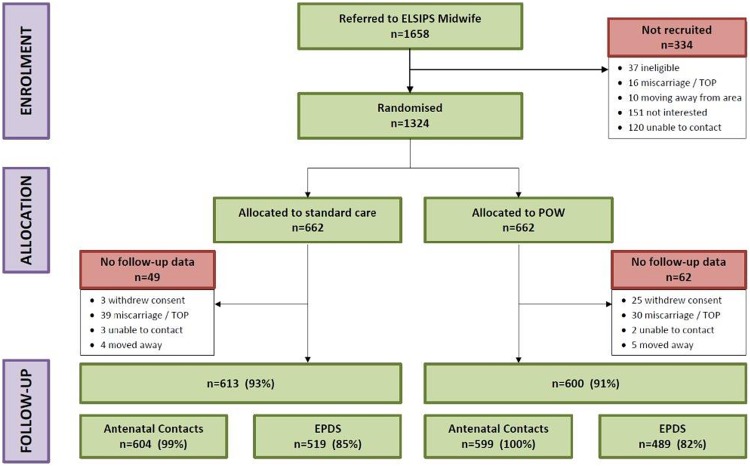
Following routine midwife systematic assessment of social risk factors, 1324 nulliparous women were assigned, using telephone randomisation, to standard maternity care, or addition of referral to a Pregnancy Outreach Worker (POW) service. Those under 16 years and teenagers recruited to the Family Nurse Partnership trial were excluded.
POWs were trained to provide individual support and case management for the women including home visiting from randomisation to 6 weeks after birth. Standard maternity care (control) included provision for referring women with social risk factors to specialist midwifery services, available to both arms.
Primary outcomes were antenatal visits attended and Edinburgh Postnatal Depression Scale (EPDS) 8-12 weeks postpartum. Prespecified, powered, subgroup comparison was among women with 2 or more social risks. Secondary outcomes included maternal and neonatal birth outcomes; maternal self-efficacy, and mother-to-infant bonding at 8-12 weeks; child development assessment at 6 weeks, breastfeeding at 6 weeks, and immunisation uptake at 4 months, all collected from routine child health systems.
Antenatal attendances were high in the standard care control and did not increase further with addition of the POW intervention (10.1 vs 10.1 (mean difference; MD) -0.00, 95% CI (95% CI -0.37 to 0.37)). In the powered subgroup of women with 2 or more social risk factors, mean EPDS (MD -0.79 (95% CI -1.56 to -0.02) was significantly better, although for all women recruited, no significant differences were seen (MD -0.59 (95% CI -1.24 to 0.06). Mother-to-infant bonding was significantly better in the intervention group for all women (MD -0.30 (95% CI -0.61 to -0.00) p=0.05), and there were no differences in other secondary outcomes.
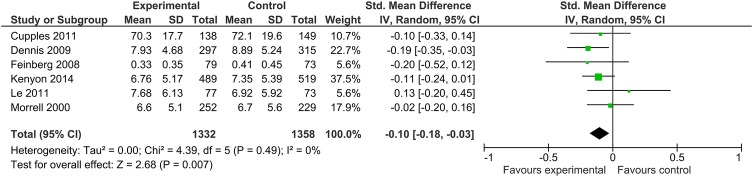
This trial demonstrates differences in depressive symptomatology with addition of the POW service in the powered subgroup of women with 2 or more social risk factors. Addition to existing evidence indicates benefit from lay interventions in preventing postnatal depression. This finding is important for women and their families given the known effect of maternal depression on longer term childhood outcomes.
ISRCTN35027323; Results.
我们探寻非专业支持在改善弱势家庭母婴结局方面有效性的证据。
前瞻性、实用性、个体随机对照试验。
英国西米德兰兹郡的3家 maternity Trusts。
在助产士对社会风险因素进行常规系统评估后,1324名未生育过的女性通过电话随机分组,分别接受标准产科护理,或在标准产科护理基础上增加转介至妊娠外展工作者(POW)服务。排除年龄在16岁以下以及参与家庭护士伙伴关系试验招募的青少年。
POW接受培训,为这些女性提供个体支持和病例管理,包括从随机分组至产后6周的家访。标准产科护理(对照组)包括将有社会风险因素的女性转介至专业助产服务,两组均可获得此项服务。
主要结局为产前检查次数以及产后8 - 12周的爱丁堡产后抑郁量表(EPDS)得分。预先设定、有统计学效力的亚组比较是在有2个或更多社会风险因素的女性中进行。次要结局包括孕产妇和新生儿出生结局;产后8 - 12周的孕产妇自我效能感和母婴联结;产后6周的儿童发育评估、产后6周的母乳喂养情况以及4个月时的疫苗接种率,所有这些数据均从常规儿童健康系统收集。
标准护理对照组的产前检查次数较高,增加POW干预后并未进一步增加(10.1对10.1(平均差;MD) - 0.00,95%置信区间(95%CI) - 0.37至0.37)。在有2个或更多社会风险因素的有统计学效力的亚组女性中,平均EPDS得分(MD - 0.79(95%CI - 1.56至 - 0.02))显著更好,尽管在所有招募的女性中未观察到显著差异(MD - 0.59(95%CI - 1.24至0.06))。对于所有女性,干预组的母婴联结显著更好(MD - 0.30(95%CI - 0.61至 - 0.00),p = 0.05),并且在其他次要结局方面没有差异。
本试验表明,在有2个或更多社会风险因素的有统计学效力的亚组女性中,增加POW服务后抑郁症状存在差异。结合现有证据表明非专业干预在预防产后抑郁方面有益。鉴于孕产妇抑郁对儿童长期结局的已知影响,这一发现对女性及其家庭很重要。
ISRCTN35027323;结果