Hegemann Nina-Sophie, Wenter Vera, Spath Sonja, Kusumo Nadia, Li Minglun, Bartenstein Peter, Fendler Wolfgang P, Stief Christian, Belka Claus, Ganswindt Ute
Department of Radiation Oncology, Klinikum der Universität, Ludwig-Maximilians-University (LMU), Marchioninistrasse 15, 81377, Munich, Germany.
Department of Nuclear Medicine, Klinikum der Universität, Ludwig-Maximilians-University (LMU), Marchioninistrasse 15, 81377, Munich, Germany.
Radiat Oncol. 2016 Mar 11;11:37. doi: 10.1186/s13014-016-0615-9.
In order to define adequate radiation portals in nodal positive prostate cancer a detailed knowledge of the anatomic lymph-node distribution is mandatory. We therefore systematically analyzed the localization of Choline PET/CT positive lymph nodes and compared it to the RTOG recommendation of pelvic CTV, as well as to previous work, the SPECT sentinel lymph node atlas.
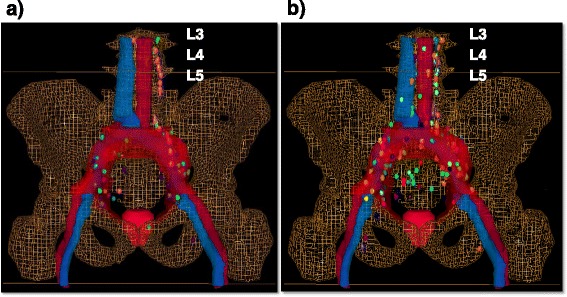
Thirty-two patients being mostly high risk patients with a PSA of 12.5 ng/ml (median) received PET/CT before any treatment. Eighty-seven patients received PET/CT for staging due to biochemical failure with a median PSA of 3.12 ng/ml. Each single PET-positive lymph node was manually contoured in a "virtual" patient dataset to achieve a 3-D visualization, resulting in an atlas of the cumulative PET positive lymph node distribution. Further the PET-positive lymph node location in each patient was assessed with regard to the existence of a potential geographic miss (i.e. PET-positive lymph nodes that would not have been treated adequately by the RTOG consensus on CTV definition of pelvic lymph nodes).
Seventy-eight and 209 PET positive lymph nodes were detected in patients with no prior treatment and in postoperative patients, respectively. The most common sites of PET positive lymph nodes in patients with no prior treatment were external iliac (32.1 %), followed by common iliac (23.1 %) and para-aortic (19.2 %). In postoperative patients the most common sites of PET positive lymph nodes were common iliac (24.9 %), followed by external iliac (23.0 %) and para-aortic (20.1 %). In patients with no prior treatment there were 34 (43.6 %) and in postoperative patients there were 77 (36.8 %) of all detected lymph nodes that would not have been treated adequately using the RTOG CTV. We compared the distribution of lymph nodes gained by Choline PET/CT to the preexisting SPECT sentinel lymph node atlas and saw an overall good congruence.
Choline PET/CT and SPECT sentinel lymph node atlas are comparable to each other. More than one-third of the PET positive lymph nodes in patients with no prior treatment and in postoperative patients would not have been treated adequately using the RTOG CTV. To reduce geographical miss, image based definition of an individual target volume is necessary.
为了确定淋巴结阳性前列腺癌的合适放疗野,必须详细了解解剖学上的淋巴结分布情况。因此,我们系统地分析了胆碱正电子发射断层扫描/计算机断层扫描(Choline PET/CT)阳性淋巴结的定位,并将其与美国放射肿瘤学会(RTOG)关于盆腔临床靶体积(CTV)的建议以及先前的研究——SPECT前哨淋巴结图谱进行比较。
32例大多为高危患者,中位前列腺特异性抗原(PSA)为12.5 ng/ml,在接受任何治疗前接受了PET/CT检查。87例因生化复发接受PET/CT分期检查的患者,中位PSA为3.12 ng/ml。在一个“虚拟”患者数据集中,对每个PET阳性淋巴结进行手动勾勒轮廓,以实现三维可视化,从而得到累积PET阳性淋巴结分布图谱。此外,针对每位患者的PET阳性淋巴结位置,评估是否存在潜在的区域遗漏(即根据RTOG关于盆腔淋巴结CTV定义的共识,未得到充分治疗的PET阳性淋巴结)。
在未接受过治疗的患者和术后患者中,分别检测到78个和209个PET阳性淋巴结。未接受过治疗的患者中,PET阳性淋巴结最常见的部位是髂外淋巴结(32.1%),其次是髂总淋巴结(23.1%)和腹主动脉旁淋巴结(19.2%)。术后患者中,PET阳性淋巴结最常见的部位是髂总淋巴结(24.9%),其次是髂外淋巴结(23.0%)和腹主动脉旁淋巴结(20.1%)。在未接受过治疗的患者中,使用RTOG CTV无法得到充分治疗的所有检测到的淋巴结有34个(43.6%);在术后患者中,这一比例为77个(36.8%)。我们将胆碱PET/CT获得的淋巴结分布与现有的SPECT前哨淋巴结图谱进行比较,发现总体一致性良好。
胆碱PET/CT和SPECT前哨淋巴结图谱具有可比性。未接受过治疗的患者和术后患者中,超过三分之一的PET阳性淋巴结使用RTOG CTV无法得到充分治疗。为了减少区域遗漏,有必要基于图像定义个体靶体积。