Dake Michael D, Ansel Gary M, Jaff Michael R, Ohki Takao, Saxon Richard R, Smouse H Bob, Machan Lindsay S, Snyder Scott A, O'Leary Erin E, Ragheb Anthony O, Zeller Thomas
From Department of Cardiothoracic Surgery, Stanford University Medical Center, Stanford, CA (M.D.D.); Department of Medicine, Ohio Health/Riverside Methodist Hospital, Columbus (G.M.A.); The Vascular Center, Massachusetts General Hospital, Boston (M.R.J.); Department of Surgery, Jikei University Hospital, Tokyo, Japan (T.O.); Department of Diagnostic Imaging and Interventional Radiology, Tri-City Medical Center, Oceanside, CA (R.R.S.); Department of Radiology, OSF St. Francis Medical Center, Peoria, IL (H.B.S.); Department of Radiology, The University of British Columbia, Vancouver, Canada (L.S.M.); Cook Research Incorporated, West Lafayette, IN (S.A.S., E.E.O'L., A.O.R.); and Department of Angiology, Herz Zentrum, Bad Krozingen, Germany (T.Z.).
Circulation. 2016 Apr 12;133(15):1472-83; discussion 1483. doi: 10.1161/CIRCULATIONAHA.115.016900. Epub 2016 Mar 11.
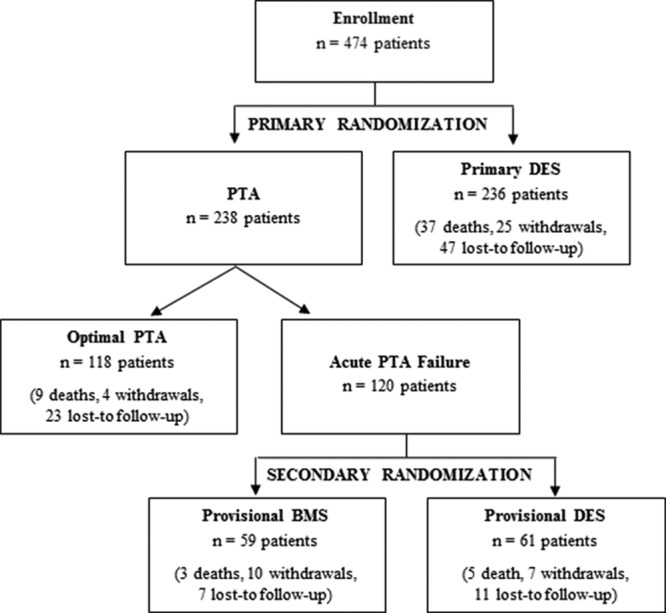
This randomized controlled trial evaluated clinical durability of Zilver PTX, a paclitaxel-coated drug-eluting stent (DES), for femoropopliteal artery lesions. Outcomes compare primary DES versus percutaneous transluminal angioplasty (PTA), overall DES (primary and provisional) versus standard care (PTA and provisional Zilver bare metal stent [BMS]), and provisional DES versus provisional BMS.
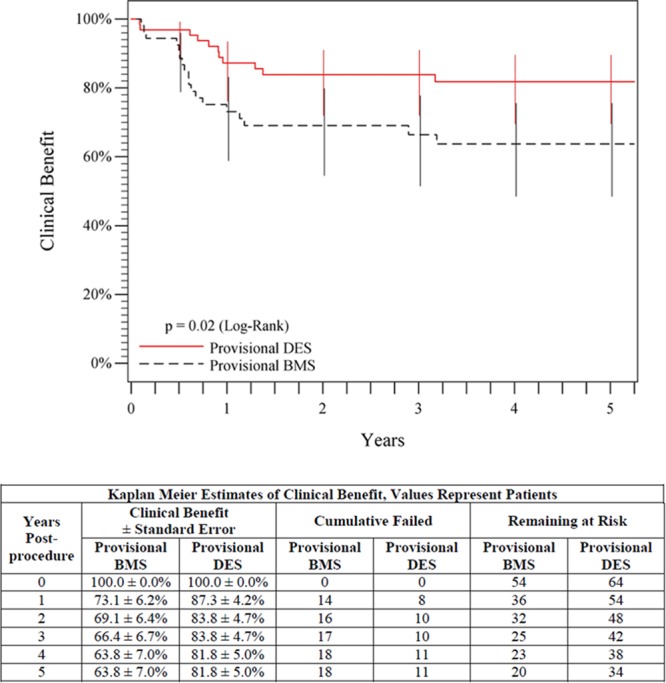
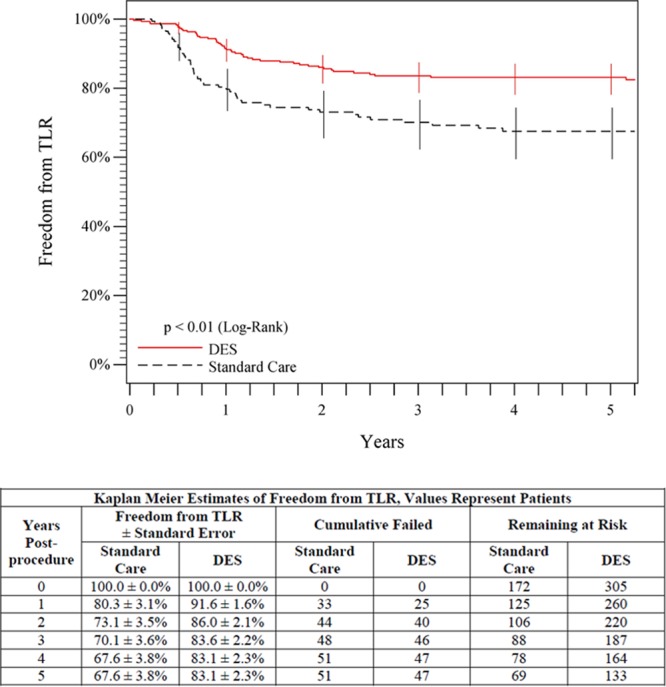
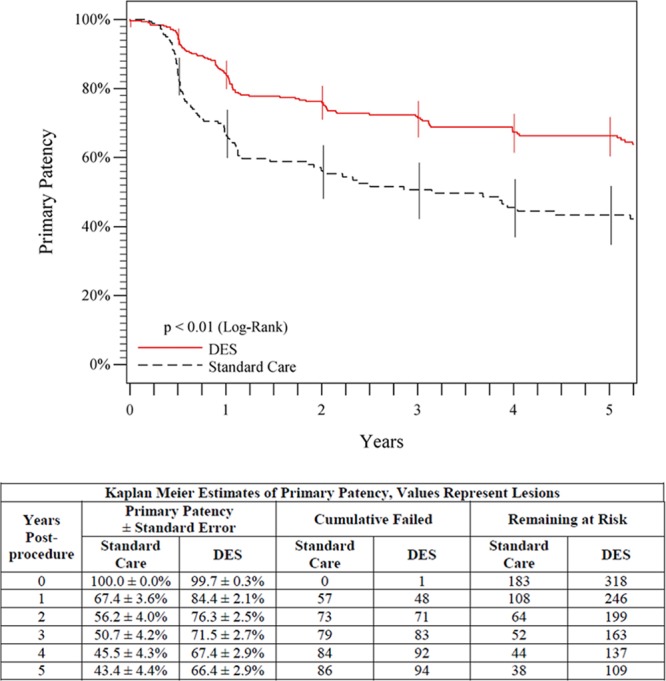
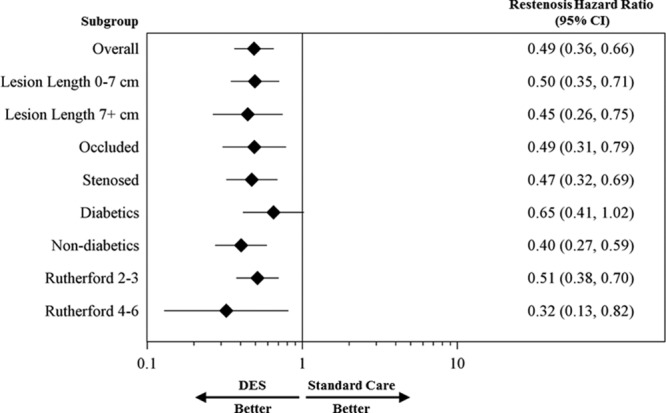
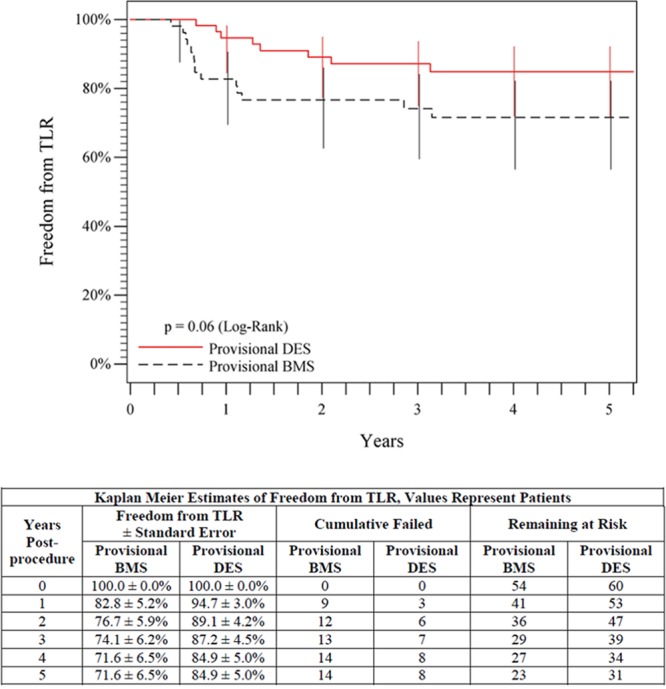
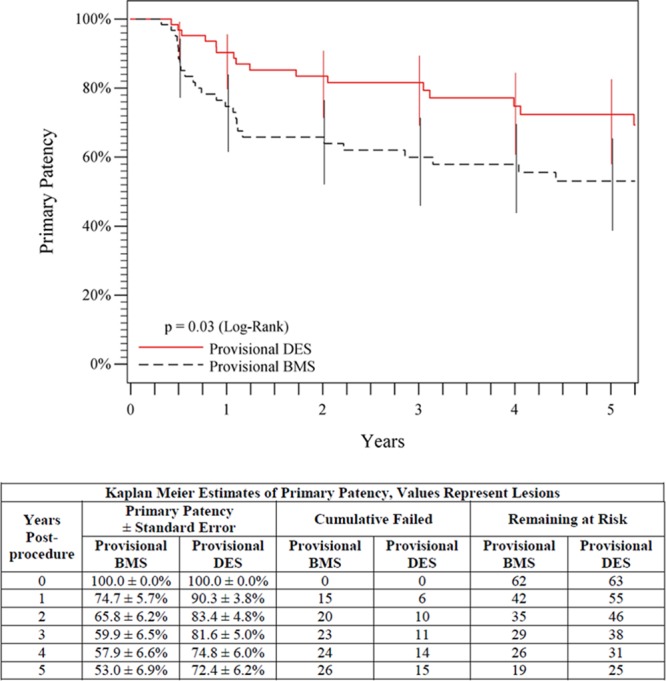
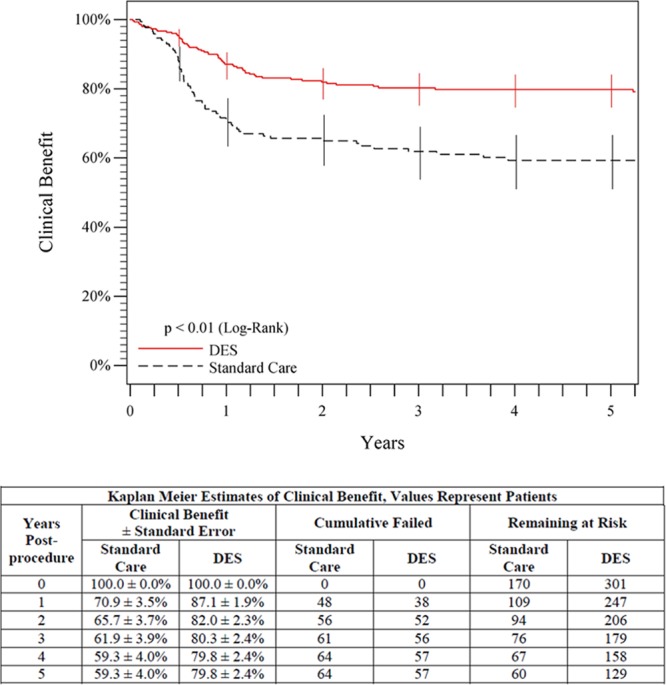
Patients with symptomatic femoropopliteal artery disease were randomly assigned to DES (n=236) or PTA (n=238). Approximately 91% had claudication; 9% had critical limb ischemia. Patients experiencing acute PTA failure underwent secondary randomization to provisional BMS (n=59) or DES (n=61). The 1-year primary end points of event-free survival and patency showed superiority of primary DES in comparison with PTA; these results were sustained through 5 years. Clinical benefit (freedom from persistent or worsening symptoms of ischemia; 79.8% versus 59.3%, P<0.01), patency (66.4% versus 43.4%, P<0.01), and freedom from reintervention (target lesion revascularization, 83.1% versus 67.6%, P<0.01) for the overall DES group were superior to standard care in nonrandomized comparisons. Similarly, clinical benefit (81.8% versus 63.8%, P=0.02), patency (72.4% versus 53.0%, P=0.03), and freedom from target lesion revascularization (84.9% versus 71.6%, P=0.06) with provisional DES were improved over provisional BMS. These results represent >40% relative risk reduction for restenosis and target lesion revascularization through 5 years for the overall DES in comparison with standard care and for provisional DES in comparison with provisional BMS.
The 5-year results from this large study provide long-term information previously unavailable regarding endovascular treatment of femoropopliteal artery disease. The Zilver PTX DES provided sustained safety and clinical durability in comparison with standard endovascular treatments.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00120406.
本随机对照试验评估了紫杉醇涂层药物洗脱支架(DES)Zilver PTX治疗股腘动脉病变的临床耐久性。比较了初次DES与经皮腔内血管成形术(PTA)、总体DES(初次和临时)与标准治疗(PTA和临时Zilver裸金属支架[BMS])以及临时DES与临时BMS的疗效。
有症状的股腘动脉疾病患者被随机分配至DES组(n = 236)或PTA组(n = 238)。约91%有间歇性跛行;9%有严重肢体缺血。急性PTA失败的患者接受二次随机分组,分为临时BMS组(n = 59)或DES组(n = 61)。1年无事件生存和通畅的主要终点显示初次DES优于PTA;这些结果持续了5年。在非随机比较中,总体DES组的临床获益(无持续或加重的缺血症状;79.8%对59.3%,P<0.01)、通畅率(66.4%对43.4%,P<0.01)和无需再次干预(靶病变血管重建,83.1%对67.6%,P<0.01)均优于标准治疗。同样,临时DES的临床获益(81.8%对63.8%,P = 0.02)、通畅率(72.4%对53.0%,P = 0.03)和无靶病变血管重建率(84.9%对71.6%,P = 0.06)均优于临时BMS。与标准治疗相比,总体DES以及与临时BMS相比,临时DES在5年内再狭窄和靶病变血管重建的相对风险降低>40%。
这项大型研究的5年结果提供了此前关于股腘动脉疾病血管内治疗的长期信息。与标准血管内治疗相比,Zilver PTX DES具有持续的安全性和临床耐久性。