Wanchoo Rimda, Jhaveri Kenar D, Deray Gilbert, Launay-Vacher Vincent
Division of Kidney Diseases and Hypertension , North Shore University Hospital and Long Island Jewish Medical Center, Hofstra NSLIJ School of Medicine , Great Neck, NY , USA.
Nephrology Department , Pitié-Salpêtrière University Hospital , Paris , France.
Clin Kidney J. 2016 Apr;9(2):245-51. doi: 10.1093/ckj/sfv149. Epub 2016 Jan 18.
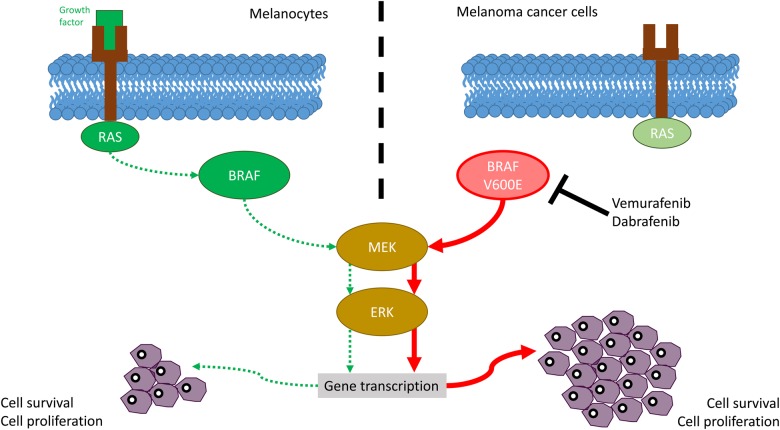
Advanced melanoma has been traditionally unresponsive to standard chemotherapy agents and used to have a dismal prognosis. Genetically targeted small-molecule inhibitors of the oncogenic BRAF V600 mutation or a downstream signaling partner (MEK mitogen-activated protein kinase) are effective treatment options for the 40-50% of melanomas that harbor mutations in BRAF. Selective BRAF and MEK inhibitors induce frequent and dramatic objective responses and markedly improve survival compared with cytotoxic chemotherapy. In the past decade after discovery of this mutation, drugs such as vemurafenib and dabrafenib have been approved by the US Food and Drug Administration (FDA) and the European Medicines Agency for the treatment of V600-mutated melanomas. While the initial trials did not signal any renal toxicities with the BRAF inhibitors, recent case reports, case series and FDA adverse reporting systems have uncovered significant nephrotoxicities with these agents. In this article, we systematically review the nephrotoxicities of these agents. Based on recently published data, it appears that there are lower rates of kidney disease and cutaneous lesions seen with dabrafenib compared with vemurafenib. The pathology reported in the few kidney biopsies done so far are suggestive of tubulo interstitial damage with an acute and chronic component. Electrolyte disorders such as hypokalemia, hyponatremia and hypophosphatemia have been reported as well. Routine monitoring of serum creatinine and electrolytes and calculation of glomerular filtration rate prior to the first administration when treating with dabrafenib and vemurafenib are essential.
传统上,晚期黑色素瘤对标准化疗药物无反应,预后很差。针对致癌性BRAF V600突变或下游信号伴侣(MEK丝裂原活化蛋白激酶)的基因靶向小分子抑制剂,是40%-50%携带BRAF突变的黑色素瘤的有效治疗选择。与细胞毒性化疗相比,选择性BRAF和MEK抑制剂能引发频繁且显著的客观反应,并显著提高生存率。在发现这种突变后的过去十年里,维莫非尼和达拉非尼等药物已获得美国食品药品监督管理局(FDA)和欧洲药品管理局批准,用于治疗V600突变的黑色素瘤。虽然最初的试验未显示BRAF抑制剂有任何肾毒性,但最近的病例报告、病例系列以及FDA不良事件报告系统发现这些药物存在显著的肾毒性。在本文中,我们系统地综述了这些药物的肾毒性。根据最近发表的数据,与维莫非尼相比,达拉非尼导致的肾病和皮肤病变发生率似乎较低。迄今为止所做的少数肾活检报告的病理结果提示存在伴有急性和慢性成分的肾小管间质损伤。也有低钾血症、低钠血症和低磷血症等电解质紊乱的报告。在用达拉非尼和维莫非尼治疗前,常规监测血清肌酐和电解质,并计算肾小球滤过率至关重要。