Martin Laura J, Roper Martha H, Grandjean Louis, Gilman Robert H, Coronel Jorge, Caviedes Luz, Friedland Jon S, Moore David A J
Laboratorio de Investigación de Enfermedades Infecciosas, Universidad Peruana Cayetano Heredia, San Martín de Porras, Lima, Peru.
Section of Infectious Diseases & Immunity & Wellcome Trust Imperial College Centre for Clinical Tropical Medicine, Imperial College London, London, UK.
BMC Med. 2016 Mar 23;14:30. doi: 10.1186/s12916-016-0576-8.
Early identification of patients with drug-resistant tuberculosis (DR-TB) increases the likelihood of treatment success and interrupts transmission. Resource-constrained settings use risk profiling to ration the use of drug susceptibility testing (DST). Nevertheless, no studies have yet quantified how many patients with DR-TB this strategy will miss.
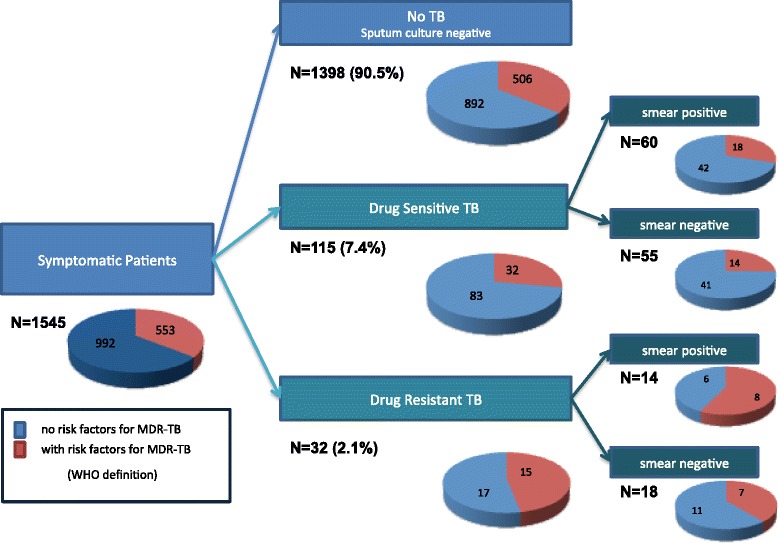
A total of 1,545 subjects, who presented to Lima health centres with possible TB symptoms, completed a clinic-epidemiological questionnaire and provided sputum samples for TB culture and DST. The proportion of drug resistance in this population was calculated and the data was analysed to demonstrate the effect of rationing tests to patients with multidrug-resistant TB (MDR-TB) risk factors on the number of tests needed and corresponding proportion of missed patients with DR-TB.
Overall, 147/1,545 (9.5%) subjects had culture-positive TB, of which 32 (21.8%) had DR-TB (MDR, 13.6%; isoniazid mono-resistant, 7.5%; rifampicin mono-resistant, 0.7%). A total of 553 subjects (35.8%) reported one or more MDR-TB risk factors; of these, 506 (91.5%; 95% CI, 88.9-93.7%) did not have TB, 32/553 (5.8%; 95% CI, 3.4-8.1%) had drug-susceptible TB, and only 15/553 (2.7%; 95% CI, 1.5-4.4%) had DR-TB. Rationing DST to those with an MDR-TB risk factor would have missed more than half of the DR-TB population (17/32, 53.2%; 95% CI, 34.7-70.9).
Rationing DST based on known MDR-TB risk factors misses an unacceptable proportion of patients with drug-resistance in settings with ongoing DR-TB transmission. Investment in diagnostic services to allow universal DST for people with presumptive TB should be a high priority.
早期识别耐多药结核病(DR-TB)患者可提高治疗成功的可能性并阻断传播。资源有限的地区采用风险评估来合理使用药敏试验(DST)。然而,尚无研究量化这种策略会遗漏多少DR-TB患者。
共有1545名因可能患有结核病症状而前往利马健康中心就诊的受试者完成了临床流行病学问卷,并提供痰液样本用于结核菌培养和DST。计算该人群中的耐药比例,并对数据进行分析,以证明对具有耐多药结核病(MDR-TB)风险因素的患者进行有限检测对所需检测数量以及相应遗漏的DR-TB患者比例的影响。
总体而言,1545名受试者中有147名(9.5%)结核菌培养呈阳性,其中32名(21.8%)患有DR-TB(耐多药,13.6%;异烟肼单耐药,7.5%;利福平单耐药,0.7%)。共有553名受试者(35.8%)报告了一项或多项MDR-TB风险因素;其中,506名(91.5%;95%置信区间,88.9-93.