Clinical Research Unit, London School of Hygiene and Tropical Medicine, London, UK.
Lancet. 2010 Oct 9;376(9748):1244-53. doi: 10.1016/S0140-6736(10)61425-0.
Control of tuberculosis in settings with high HIV prevalence is a pressing public health priority. We tested two active case-finding strategies to target long periods of infectiousness before diagnosis, which is typical of HIV-negative tuberculosis and is a key driver of transmission.
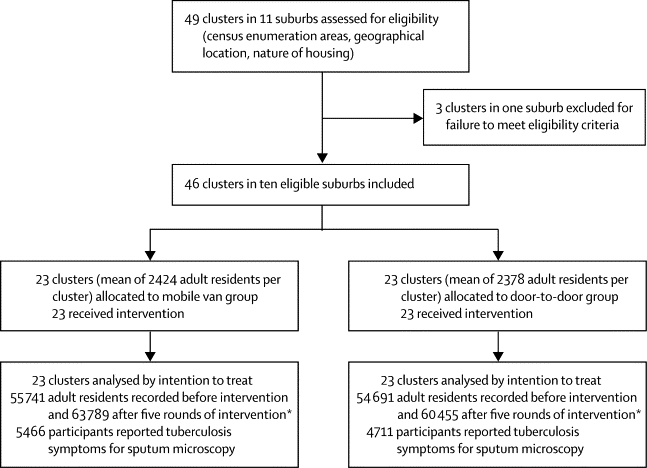
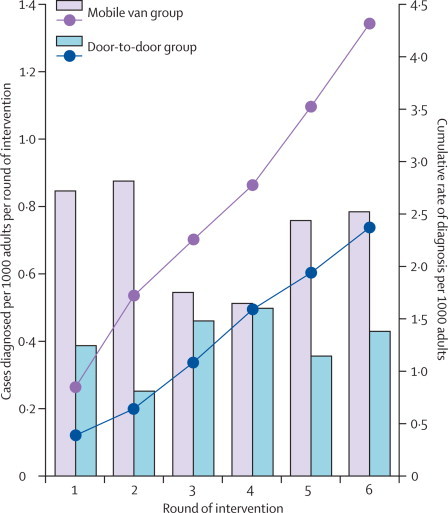
Clusters of neighbourhoods in the high-density residential suburbs of Harare, Zimbabwe, were randomised to receive six rounds of active case finding at 6-monthly intervals by either mobile van or door-to-door visits. Randomisation was done by selection of discs of two colours from an opaque bag, with one disc to represent every cluster, and one colour allocated to each intervention group before selection began. In both groups, adult (≥16 years) residents volunteering chronic cough (≥2 weeks) had two sputum specimens collected for fluorescence microscopy. Community health workers and cluster residents were not masked to intervention allocation, but investigators and laboratory staff were masked to allocation until final analysis. The primary outcome was the cumulative yield of smear-positive tuberculosis per 1000 adult residents, compared between intervention groups; analysis was by intention to treat. The secondary outcome was change in prevalence of culture-positive tuberculosis from before intervention to before round six of intervention in 12% of randomly selected households from the two intervention groups combined; analysis was based on participants who provided sputum in the two prevalence surveys. This trial is registered, number ISRCTN84352452.
46 study clusters were identified and randomly allocated equally between intervention groups, with 55 741 adults in the mobile van group and 54,691 in the door-to-door group at baseline. HIV prevalence was 21% (1916/9060) and in the 6 months before intervention the smear-positive case notification rate was 2·8 per 1000 adults per year. The trial was completed as planned with no adverse events. The mobile van detected 255 smear-positive patients from 5466 participants submitting sputum compared with 137 of 4711 participants identified through door-to-door visits (adjusted risk ratio 1·48, 95% CI 1·11-1·96, p=0·0087). The overall prevalence of culture-positive tuberculosis declined from 6·5 per 1000 adults (95% CI 5·1-8·3) to 3·7 per 1000 adults (2·6-5·0; adjusted risk ratio 0·59, 95% CI 0·40-0·89, p=0·0112).
Wide implementation of active case finding, particularly with a mobile van approach, could have rapid effects on tuberculosis transmission and disease.
Wellcome Trust.
在 HIV 流行率较高的环境中控制结核病是一项紧迫的公共卫生重点。我们测试了两种主动病例发现策略,以针对诊断前的长时间传染性,这是 HIV 阴性结核病的典型特征,也是传播的关键驱动因素。
津巴布韦哈拉雷高密度住宅区的街区集群被随机分配,每隔 6 个月接受 6 轮主动病例发现,方法是通过移动面包车或挨家挨户访问。通过从不透明袋中选择两个颜色的圆盘进行随机分组,每个圆盘代表一个集群,并且在开始选择之前为每个干预组分配一种颜色。在两组中,自愿患有慢性咳嗽(≥2 周)的成年(≥16 岁)居民采集两份痰标本进行荧光显微镜检查。社区卫生工作者和集群居民未对干预分配进行掩蔽,但调查人员和实验室工作人员在最终分析之前对分配进行了掩蔽。主要结局是每 1000 名成年居民中每 1000 名成年居民中累计发现涂片阳性结核病的人数,与干预组之间进行比较;分析为意向治疗。次要结局是在两轮干预前的 12%的随机选择家庭中,从两组联合的 12%的随机选择家庭中,比较两组干预前和第六轮干预前培养阳性结核病的患病率变化;分析基于在两次患病率调查中提供痰液的参与者。这项试验已注册,编号为 ISRCTN84352452。
确定了 46 个研究集群,并在干预组之间平均随机分配,移动面包车组有 55741 名成年人,门到门组有 54691 名成年人作为基线。HIV 流行率为 21%(1916/9060),在干预前的 6 个月中,每年每 1000 名成年人中报告的涂片阳性病例数为 2.8。该试验按计划完成,没有不良事件。移动面包车从 5466 名提交痰液的参与者中检测到 255 名涂片阳性患者,而通过家访发现的 4711 名参与者中发现了 137 名(调整风险比 1.48,95%CI 1.11-1.96,p=0.0087)。总体培养阳性结核病的患病率从每 1000 名成年人 6.5 人(95%CI 5.1-8.3)降至每 1000 名成年人 3.7 人(2.6-5.0;调整风险比 0.59,95%CI 0.40-0.89,p=0.0112)。
广泛实施主动病例发现,特别是采用移动面包车方法,可能会对结核病传播和疾病产生快速影响。
惠康信托基金会。