Duta Ciprian, Pantea Stelian, Lazar Caius, Salim Abdullah, Barjica Daniela
Surgical Clinic 2, University of Medicine and Pharmacy, "V. Babes," Timisoara, Romania.
JSLS. 2016 Jan-Mar;20(1). doi: 10.4293/JSLS.2016.00002.
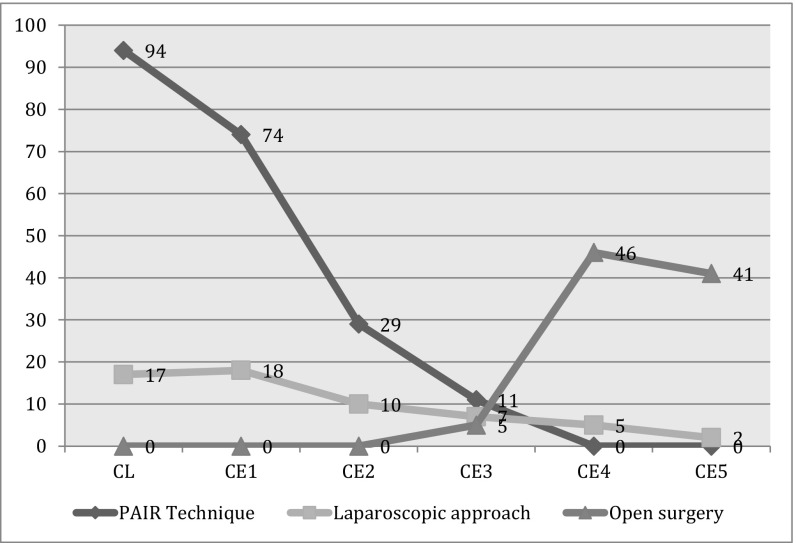
Open surgery has been the mainstay treatment for liver hydatidosis in the past. Today, for treatment of simple and uncomplicated cysts, we have a variety of choices: antihelmintic therapy, the PAIR (puncture, aspiration, injection, and respiration) technique, and the laparoscopic approach. We reviewed our series of 267 cases of hepatic hydatidosis submitted to surgery over a period of 20 years, from 1995 through 2014, comparing the results of these minimally invasive treatments.
In 92 patients (25.7% of cases) who presented with complicated liver hydatid cysts, we performed open surgery. In 16.4% of cases (59 patients), we used a laparoscopic approach, and in 208 patients (57.9% of cases), we used the PAIR technique. All patients were monitored after surgery for a mean of 61.7 months (range, 16-127). Postoperative follow-up consisted of clinical examination, laboratory investigation, abdominal ultrasound, and magnetic resonance imaging.
Almost all patients (198, 95.2%) treated with the PAIR technique and 55 patients (93.2%) treated with the laparoscopic approach were cured. Six patients (2.8%) from the echo-guided puncture group had to undergo a repeat of the procedure because the cavity did not disappear after 2 years. In 4 patients (2%), we performed open surgery for 2 biliary fistulas and 2 hepatic abscesses. Four patients from the laparoscopic group needed additional procedures. Open surgery was necessary in 2 patients for a recurrence after 2 years; 1 patient had developed a liver abscess and the other had a biliary fistula.
In conclusion, open surgery remains the viable option for complicated cysts, with biliary communication, with multiple daughter vesicles, or with calcified walls. For simple, uncomplicated hydatid cysts, both methods (the PAIR technique and laparoscopic procedure) are safe and efficient, with very good results and low morbidity rates.
过去,开放手术一直是肝包虫病的主要治疗方法。如今,对于单纯性和非复杂性囊肿的治疗,我们有多种选择:抗蠕虫治疗、PAIR(穿刺、抽吸、注射和再抽吸)技术以及腹腔镜手术。我们回顾了1995年至2014年20年间接受手术治疗的267例肝包虫病患者的病例系列,比较了这些微创治疗的结果。
92例(占病例的25.7%)患有复杂性肝包虫囊肿的患者接受了开放手术。59例(占病例的16.4%)患者采用了腹腔镜手术,208例(占病例的57.9%)患者采用了PAIR技术。所有患者术后平均随访61.7个月(范围16 - 127个月)。术后随访包括临床检查、实验室检查、腹部超声和磁共振成像。
几乎所有接受PAIR技术治疗的患者(198例,95.2%)和接受腹腔镜手术治疗的55例患者(93.2%)均治愈。超声引导穿刺组有6例患者(2.8%)因2年后囊肿腔未消失而需再次进行该操作。4例患者(2%)因2例胆瘘和2例肝脓肿接受了开放手术。腹腔镜组有4例患者需要额外的手术。2例患者在2年后复发需要进行开放手术;1例患者发生了肝脓肿,另1例患者出现了胆瘘。
总之,对于伴有胆道相通、多个子囊或钙化壁的复杂性囊肿,开放手术仍是可行的选择。对于单纯性、非复杂性包虫囊肿,PAIR技术和腹腔镜手术这两种方法都是安全有效的,效果良好且发病率低。