Michler Robert E, Smith Peter K, Parides Michael K, Ailawadi Gorav, Thourani Vinod, Moskowitz Alan J, Acker Michael A, Hung Judy W, Chang Helena L, Perrault Louis P, Gillinov A Marc, Argenziano Michael, Bagiella Emilia, Overbey Jessica R, Moquete Ellen G, Gupta Lopa N, Miller Marissa A, Taddei-Peters Wendy C, Jeffries Neal, Weisel Richard D, Rose Eric A, Gammie James S, DeRose Joseph J, Puskas John D, Dagenais François, Burks Sandra G, El-Hamamsy Ismail, Milano Carmelo A, Atluri Pavan, Voisine Pierre, O'Gara Patrick T, Gelijns Annetine C
From the Department of Cardiothoracic and Vascular Surgery, Montefiore Medical Center-Albert Einstein College of Medicine (R.E.M., J.J.D.), the International Center for Health Outcomes and Innovation Research (InCHOIR), Department of Population Health Science and Policy, Icahn School of Medicine at Mount Sinai (M.K.P., A.J.M., H.L.C., E.B., J.R.O., E.G.M., L.N.G., A.C.G.), the Division of Cardiothoracic Surgery, Department of Surgery, College of Physicians and Surgeons, Columbia University (M.A.), and the Department of Cardiac Surgery, Mount Sinai Health System (E.A.R., J.D.P.) - all in New York; the Division of Cardiovascular and Thoracic Surgery, Department of Surgery, Duke University Medical Center, Durham, NC (P.K.S., C.A.M.); the Division of Thoracic and Cardiovascular Surgery, University of Virginia School of Medicine, Charlottesville (G.A., S.G.B.); the Clinical Research Unit, Division of Cardiothoracic Surgery, Emory University School of Medicine, Atlanta (V.T.); the Department of Surgery, Division of Cardiovascular Surgery, University of Pennsylvania School of Medicine, Philadelphia (M.A.A., P.A.); the Division of Cardiology, Massachusetts General Hospital (J.W.H.), and the Cardiovascular Division, Brigham and Women's Hospital (P.T.O.) - both in Boston; Montreal Heart Institute, University of Montreal, Montreal (L.P.P., I.E.-H.), Peter Munk Cardiac Centre and Division of Cardiovascular Surgery, Toronto General Hospital, University Health Network and the Division of Cardiac Surgery, University of Toronto, Toronto (R.D.W.), and Institut Universitaire de Cardiologie de Québec, Hôpital Laval, Quebec, QC (F.D., P.V.) - all in Canada; the Department of Thoracic and Cardiovascular Surgery, Cleveland Clinic Foundation, Cleveland (A.M.G.); and the Division of Cardiovascular Sciences (M.A.M., W.C.T.-P.) and Office of Biostatistics Research (N.J.), National Heart, Lung, and Blood Institute, Bethesda, and the Department of Surgery, University of Maryland Medical Cent
N Engl J Med. 2016 May 19;374(20):1932-41. doi: 10.1056/NEJMoa1602003. Epub 2016 Apr 3.
In a trial comparing coronary-artery bypass grafting (CABG) alone with CABG plus mitral-valve repair in patients with moderate ischemic mitral regurgitation, we found no significant difference in the left ventricular end-systolic volume index (LVESVI) or survival after 1 year. Concomitant mitral-valve repair was associated with a reduced prevalence of moderate or severe mitral regurgitation, but patients had more adverse events. We now report 2-year outcomes.
We randomly assigned 301 patients to undergo either CABG alone or the combined procedure. Patients were followed for 2 years for clinical and echocardiographic outcomes.
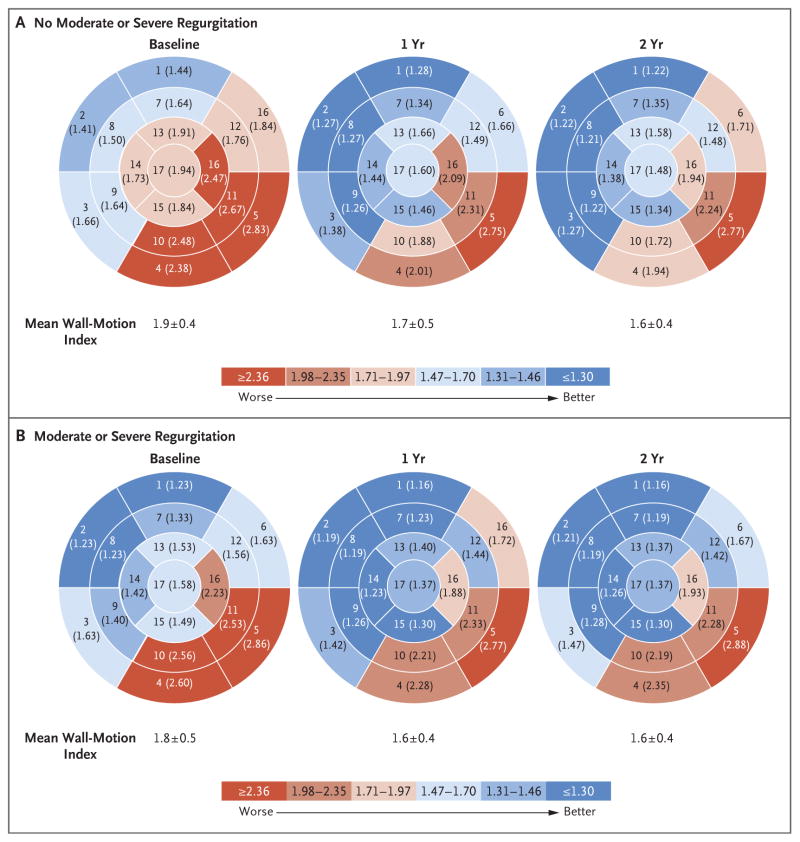
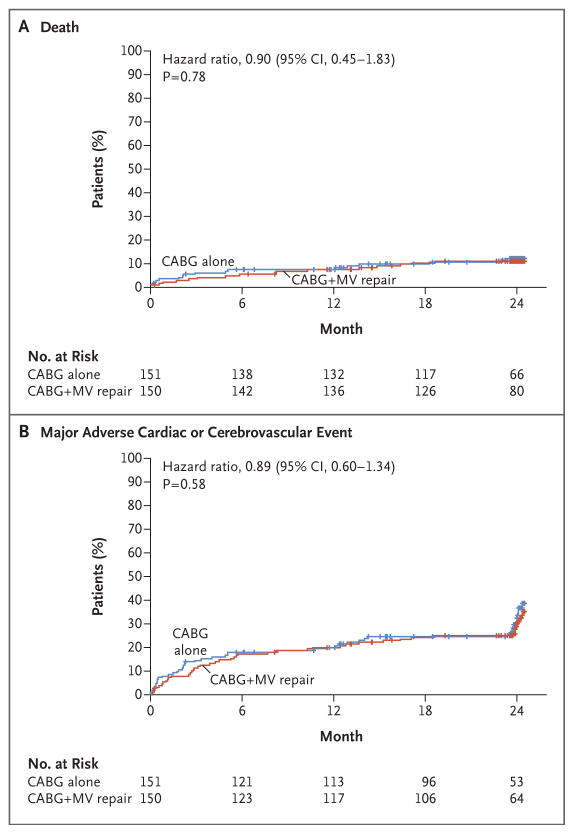
At 2 years, the mean (±SD) LVESVI was 41.2±20.0 ml per square meter of body-surface area in the CABG-alone group and 43.2±20.6 ml per square meter in the combined-procedure group (mean improvement over baseline, -14.1 ml per square meter and -14.6 ml per square meter, respectively). The rate of death was 10.6% in the CABG-alone group and 10.0% in the combined-procedure group (hazard ratio in the combined-procedure group, 0.90; 95% confidence interval, 0.45 to 1.83; P=0.78). There was no significant between-group difference in the rank-based assessment of the LVESVI (including death) at 2 years (z score, 0.38; P=0.71). The 2-year rate of moderate or severe residual mitral regurgitation was higher in the CABG-alone group than in the combined-procedure group (32.3% vs. 11.2%, P<0.001). Overall rates of hospital readmission and serious adverse events were similar in the two groups, but neurologic events and supraventricular arrhythmias remained more frequent in the combined-procedure group.
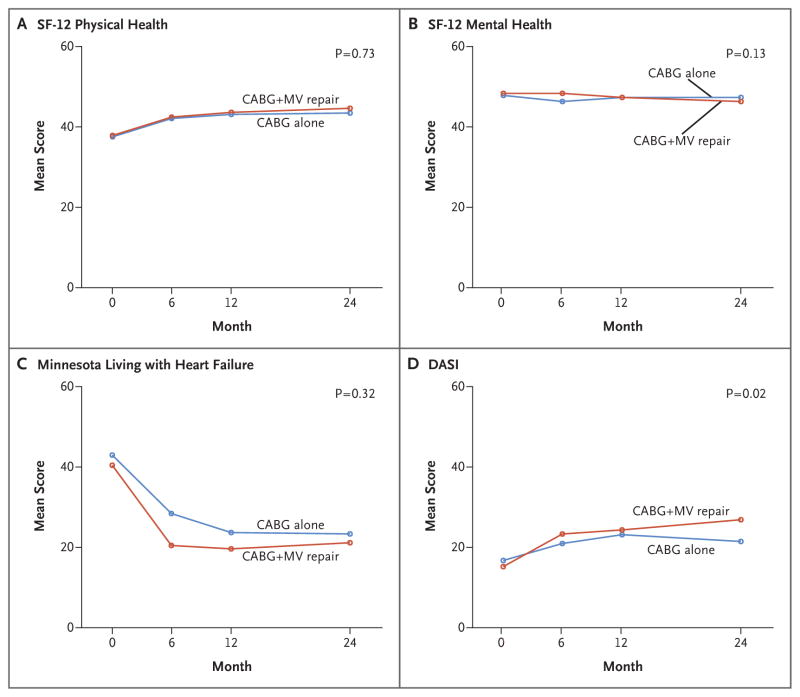
In patients with moderate ischemic mitral regurgitation undergoing CABG, the addition of mitral-valve repair did not lead to significant differences in left ventricular reverse remodeling at 2 years. Mitral-valve repair provided a more durable correction of mitral regurgitation but did not significantly improve survival or reduce overall adverse events or readmissions and was associated with an early hazard of increased neurologic events and supraventricular arrhythmias. (Funded by the National Institutes of Health and Canadian Institutes of Health Research; ClinicalTrials.gov number, NCT00806988.).
在一项比较单纯冠状动脉旁路移植术(CABG)与CABG联合二尖瓣修复术治疗中度缺血性二尖瓣反流患者的试验中,我们发现左心室收缩末期容积指数(LVESVI)或1年后的生存率无显著差异。二尖瓣联合修复术与中度或重度二尖瓣反流患病率降低相关,但患者有更多不良事件。我们现在报告2年的结果。
我们将301例患者随机分为单纯接受CABG或联合手术组。对患者进行2年的随访,观察临床和超声心动图结果。
2年时,单纯CABG组的平均(±标准差)LVESVI为每平方米体表面积41.2±20.0 ml,联合手术组为每平方米43.2±20.6 ml(相对于基线的平均改善分别为每平方米-14.1 ml和-14.6 ml)。单纯CABG组的死亡率为10.6%,联合手术组为10.0%(联合手术组的风险比为0.90;95%置信区间为0.45至1.83;P = 0.78)。2年时基于秩次的LVESVI评估(包括死亡)在组间无显著差异(z值为0.38;P = 0.71)。单纯CABG组中度或重度二尖瓣反流的2年发生率高于联合手术组(32.3%对11.2%,P<0.001)。两组的总体再入院率和严重不良事件发生率相似,但联合手术组的神经系统事件和室上性心律失常仍然更频繁。
在接受CABG的中度缺血性二尖瓣反流患者中,增加二尖瓣修复术在2年时并未导致左心室逆向重构有显著差异。二尖瓣修复术能更持久地纠正二尖瓣反流,但并未显著提高生存率或减少总体不良事件或再入院率,且与神经系统事件和室上性心律失常增加的早期风险相关。(由美国国立卫生研究院和加拿大卫生研究院资助;ClinicalTrials.gov编号,NCT00806988。)