Abdel-Wahab N, Lopez-Olivo M A, Pinto-Patarroyo G P, Suarez-Almazor M E
Section of Rheumatology and Clinical Immunology, Department of General Internal Medicine, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Rheumatology and Rehabilitation Department, Assiut University Hospitals, Assiut, Egypt.
Lupus. 2016 Dec;25(14):1520-1531. doi: 10.1177/0961203316640912. Epub 2016 Apr 7.
The objective of this study was to conduct a systematic review of case reports documenting the development of antiphospholipid syndrome or antiphospholipid syndrome-related features after an infection.
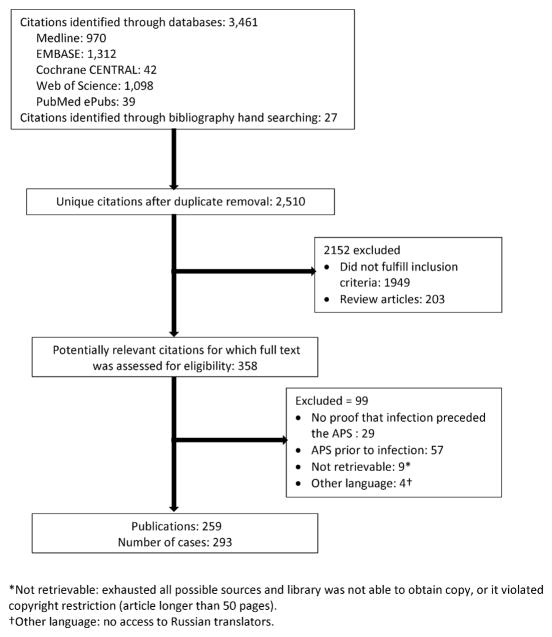
We searched Medline, EMBASE, Web of Science, PubMed ePubs, and The Cochrane Library - CENTRAL through March 2015 without restrictions. Studies reporting cases of antiphospholipid syndrome or antiphospholipid syndrome-related features following an infection were included.
Two hundred and fifty-nine publications met inclusion criteria, reporting on 293 cases. Three different groups of patients were identified; group 1 included patients who fulfilled the criteria for definitive antiphospholipid syndrome (24.6%), group 2 included patients who developed transient antiphospholipid antibodies with thromboembolic phenomena (43.7%), and group 3 included patients who developed transient antiphospholipid antibodies without thromboembolic events (31.7%). The most common preceding infection was viral (55.6%). In cases that developed thromboembolic events Human immunodeficiency and Hepatitis C viruses were the most frequently reported. Parvovirus B19 was the most common in cases that developed antibodies without thromboembolic events. Hematological manifestations and peripheral thrombosis were the most common clinical manifestations. Positive anticardiolipin antibodies were the most frequent antibodies reported, primarily coexisting IgG and IgM isotypes. Few patients in groups 1 and 2 had persistent antiphospholipid antibodies for more than 6 months. Outcome was variable with some cases reporting persistent antiphospholipid syndrome features and others achieving complete resolution of clinical events.
Development of antiphospholipid antibodies with all traditional manifestations of antiphospholipid syndrome were observed after variety of infections, most frequently after chronic viral infections with Human immunodeficiency and Hepatitis C. The causal relationship between infection and antiphospholipid syndrome cannot be established, but the possible contribution of various infections in the pathogenesis of antiphospholipid syndrome need further longitudinal and controlled studies to establish the incidence, and better quantify the risk and the outcomes of antiphospholipid-related events after infection.
本研究旨在对记录感染后抗磷脂综合征或抗磷脂综合征相关特征发生情况的病例报告进行系统评价。
我们检索了截至2015年3月的Medline、EMBASE、科学网、PubMed电子出版物和考克兰图书馆 - 中心库,检索无限制。纳入报告感染后抗磷脂综合征或抗磷脂综合征相关特征病例的研究。
259篇出版物符合纳入标准,报告了293例病例。确定了三组不同的患者;第1组包括符合确定性抗磷脂综合征标准的患者(24.6%),第2组包括出现伴有血栓栓塞现象的短暂性抗磷脂抗体的患者(43.7%),第3组包括出现无血栓栓塞事件的短暂性抗磷脂抗体的患者(31.7%)。最常见的前驱感染是病毒感染(55.6%)。在发生血栓栓塞事件的病例中,人类免疫缺陷病毒和丙型肝炎病毒是最常报告的。在出现无血栓栓塞事件的抗体的病例中,细小病毒B19最为常见。血液学表现和外周血栓形成是最常见的临床表现。抗心磷脂抗体阳性是最常报告的抗体,主要是IgG和IgM同种型共存。第1组和第2组中很少有患者抗磷脂抗体持续超过6个月。结果各不相同,一些病例报告有持续性抗磷脂综合征特征,而另一些病例临床事件完全缓解。
在各种感染后,观察到出现具有抗磷脂综合征所有传统表现的抗磷脂抗体,最常见于人类免疫缺陷病毒和丙型肝炎病毒的慢性病毒感染后。感染与抗磷脂综合征之间的因果关系尚不能确定,但各种感染在抗磷脂综合征发病机制中的可能作用需要进一步的纵向和对照研究来确定发病率,并更好地量化感染后抗磷脂相关事件的风险和结局。