Department of Pediatrics, University of Tennessee Health Science Center, Memphis, TN, USA; Department of Pediatrics, Le Bonheur Children's Hospital, Memphis, TN, USA; Children's Foundation Research Institute at Le Bonheur Children's Hospital, Memphis, TN, USA.
Pain Neurobiology Laboratory, Stanford University , Palo Alto, CA , USA.
Front Pediatr. 2016 Mar 31;4:31. doi: 10.3389/fped.2016.00031. eCollection 2016.
Lung injury activates multiple pro-inflammatory pathways, including neutrophils, epithelial, and endothelial injury, and coagulation factors leading to acute respiratory distress syndrome (ARDS). Low-dose methylprednisolone therapy (MPT) improved oxygenation and ventilation in early pediatric ARDS without altering duration of mechanical ventilation or mortality. We evaluated the effects of MPT on biomarkers of endothelial [Ang-2 and soluble intercellular adhesion molecule-1 (sICAM-1)] or epithelial [soluble receptor for activated glycation end products (sRAGE)] injury, neutrophil activation [matrix metalloproteinase-8 (MMP-8)], and coagulation (plasminogen activator inhibitor-1).
Double-blind, placebo-controlled randomized trial.
Tertiary-care pediatric intensive care unit (ICU).
Mechanically ventilated children (0-18 years) with early ARDS.
Blood samples were collected on days 0 (before MPT), 7, and 14 during low-dose MPT (n = 17) vs. placebo (n = 18) therapy. The MPT group received a 2-mg/kg loading dose followed by 1 mg/kg/day continuous infusions from days 1 to 7, tapered off over 7 days; placebo group received equivalent amounts of 0.9% saline. We analyzed plasma samples using a multiplex assay for five biomarkers of ARDS. Multiple regression models were constructed to predict associations between changes in biomarkers and the clinical outcomes reported earlier, including P/F ratio on days 8 and 9, plateau pressure on days 1 and 2, PaCO2 on days 2 and 3, racemic epinephrine following extubation, and supplemental oxygen at ICU discharge.
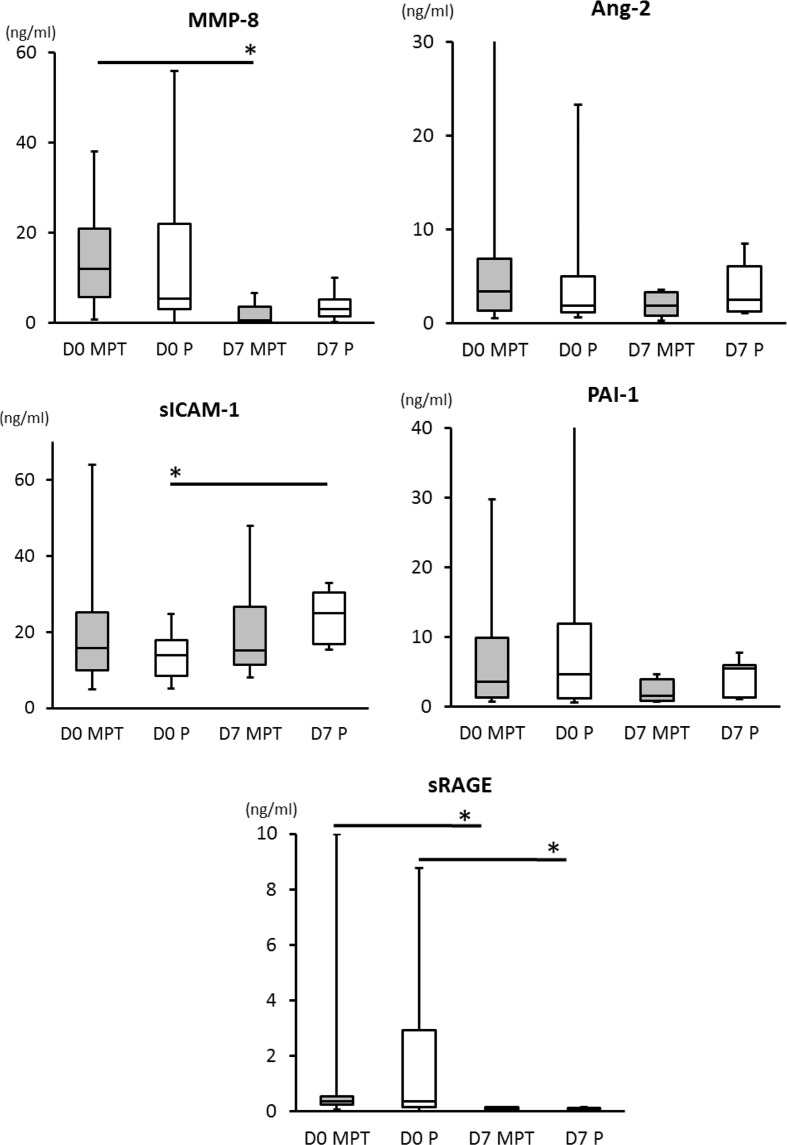
No differences occurred in biomarker concentrations between the groups on day 0. On day 7, reduction in MMP-8 levels (p = 0.0016) occurred in the MPT group, whereas increases in sICAM-1 levels (p = 0.0005) occurred in the placebo group (no increases in sICAM-1 in the MPT group). sRAGE levels decreased in both MPT and placebo groups (p < 0.0001) from day 0 to day 7. On day 7, sRAGE levels were positively correlated with MPT group PaO2/FiO2 ratios on day 8 (r = 0.93, p = 0.024). O2 requirements at ICU transfer positively correlated with day 7 MMP-8 (r = 0.85, p = 0.016) and Ang-2 levels (r = 0.79, p = 0.036) in the placebo group and inversely correlated with day 7 sICAM-1 levels (r = -0.91, p = 0.005) in the MPT group.
Biomarkers selected from endothelial, epithelial, or intravascular factors can be correlated with clinical endpoints in pediatric ARDS. For example, MPT could reduce neutrophil activation (⇓MMP-8), decrease endothelial injury (⇔sICAM-1), and allow epithelial recovery (⇓sRAGE). Large ARDS clinical trials should develop similar frameworks.
https://clinicaltrials.gov, NCT01274260.
肺损伤激活了多种促炎途径,包括中性粒细胞、上皮和内皮损伤以及凝血因子,导致急性呼吸窘迫综合征(ARDS)。小剂量甲基强的松龙治疗(MPT)可改善儿科 ARDS 患者的氧合和通气,而不改变机械通气时间或死亡率。我们评估了 MPT 对内皮[血管生成素-2 和可溶性细胞间黏附分子-1(sICAM-1)]或上皮[可溶性晚期糖基化终产物受体(sRAGE)]损伤、中性粒细胞活化[基质金属蛋白酶-8(MMP-8)]和凝血(纤溶酶原激活物抑制剂-1)的生物标志物的影响。
双盲、安慰剂对照随机试验。
三级儿科重症监护病房(ICU)。
有早期 ARDS 的机械通气患儿(0-18 岁)。
在低剂量 MPT(n=17)与安慰剂(n=18)治疗期间,于第 0 天(MPT 前)、第 7 天和第 14 天采集血样。MPT 组给予 2mg/kg 的负荷剂量,然后从第 1 天至第 7 天给予 1mg/kg/天的持续输注,7 天内逐渐减少;安慰剂组给予等量的 0.9%生理盐水。我们使用多重分析测定法分析了五个 ARDS 生物标志物的血浆样本。建立了多元回归模型,以预测生物标志物变化与之前报告的临床结局之间的关系,包括第 8 天和第 9 天的 PaO2/FiO2 比值、第 1 天和第 2 天的平台压、第 2 天和第 3 天的 PaCO2、拔管后去甲肾上腺素和 ICU 出院时的补充氧。
两组在第 0 天的生物标志物浓度无差异。第 7 天,MPT 组 MMP-8 水平降低(p=0.0016),而安慰剂组 sICAM-1 水平升高(p=0.0005)(MPT 组 sICAM-1 无升高)。sRAGE 水平从第 0 天到第 7 天在 MPT 和安慰剂组均降低(p<0.0001)。第 7 天,sRAGE 水平与 MPT 组第 8 天的 PaO2/FiO2 比值呈正相关(r=0.93,p=0.024)。ICU 转院时的氧需求与第 7 天 MMP-8(r=0.85,p=0.016)和 Ang-2 水平(r=0.79,p=0.036)在安慰剂组呈正相关,与 MPT 组第 7 天 sICAM-1 水平呈负相关(r=-0.91,p=0.005)。
从内皮、上皮或血管内因素中选择的生物标志物可以与儿科 ARDS 的临床终点相关。例如,MPT 可以减少中性粒细胞的激活(↓MMP-8),降低内皮损伤(↔sICAM-1),并允许上皮恢复(↓sRAGE)。大型 ARDS 临床试验应制定类似的框架。