Yang Jie, Tang Grace, Zhang Pengpeng, Hunt Margie, Lim Seng B, LoSasso Thomas, Mageras Gig
Memorial Sloan Kettering Cancer Center.
J Appl Clin Med Phys. 2016 Mar 8;17(2):3-13. doi: 10.1120/jacmp.v17i2.4989.
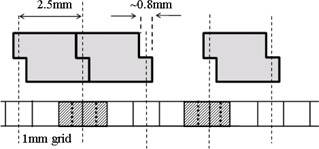
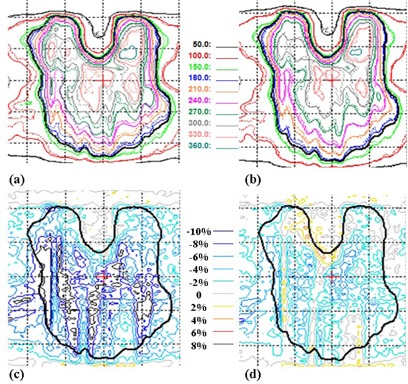
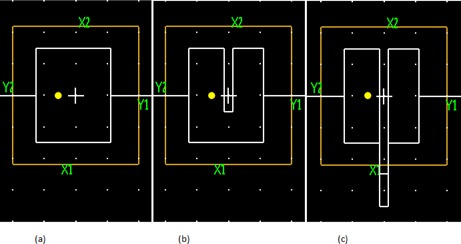
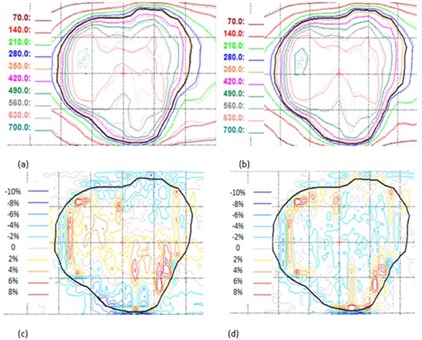
Hypofractionated treatments generally increase the complexity of a treatment plan due to the more stringent constraints of normal tissues and target coverage. As a result, treatment plans contain more modulated MLC motions that may require extra efforts for accurate dose calculation. This study explores methods to minimize the differences between in-house dose calculation and actual delivery of hypofractionated volumetric-modulated arc therapy (VMAT), by focusing on arc approximation and tongue-and-groove (TG) modeling. For dose calculation, the continuous delivery arc is typically approximated by a series of static beams with an angular spacing of 2°. This causes significant error when there is large MLC movement from one beam to the next. While increasing the number of beams will minimize the dose error, calculation time will increase significantly. We propose a solution by inserting two additional apertures at each of the beam angle for dose calculation. These additional apertures were interpolated at two-thirds' degree before and after each beam. Effectively, there were a total of three MLC apertures at each beam angle, and the weighted average fluence from the three apertures was used for calculation. Because the number of beams was kept the same, calculation time was only increased by about 6%-8%. For a lung plan, areas of high local dose differences (> 4%) between film measurement and calculation with one aperture were significantly reduced in calculation with three apertures. Ion chamber measurement also showed similar results, where improvements were seen with calculations using additional apertures. Dose calculation accuracy was further improved for TG modeling by developing a sampling method for beam fluence matrix. Single element point sampling for fluence transmitted through MLC was used for our fluence matrix with 1 mm resolution. For Varian HDMLC, grid alignment can cause fluence sampling error. To correct this, transmission volume averaging was applied. For three paraspinal HDMLC cases, the average dose difference was greatly reduced in film and calculation comparisons with our new approach. The gamma (3%, 3 mm) pass rates have improved significantly from 74.1%, 90.0%, and 90.4% to 99.2%, 97.9%, and 97.3% for three cases, for calculation without volume averaging and calculation with volume averaging, respectively. Our results indicate that more accurate MLC leaf position and transmission sampling can improve accuracy and agreement between calculation and measurement, and are particularly important for hypofractionated VMAT that consists of large MLC movement.
由于正常组织和靶区覆盖的限制更为严格,大分割治疗通常会增加治疗计划的复杂性。因此,治疗计划包含更多的调强多叶准直器(MLC)运动,这可能需要额外的努力来进行精确的剂量计算。本研究通过关注弧形近似和舌槽(TG)建模,探索了最小化内部剂量计算与大分割容积调强弧形治疗(VMAT)实际交付之间差异的方法。对于剂量计算,连续的弧形照射通常由一系列角度间隔为2°的静态射束近似。当MLC从一个射束到下一个射束有较大移动时,这会导致显著误差。虽然增加射束数量将使剂量误差最小化,但计算时间将显著增加。我们提出了一种解决方案,即在每个射束角度插入两个额外的孔径用于剂量计算。这些额外的孔径在每个射束前后三分之二度处进行插值。实际上,每个射束角度共有三个MLC孔径,并且使用这三个孔径的加权平均注量进行计算。由于射束数量保持不变,计算时间仅增加约6%-8%。对于肺部计划,在使用一个孔径进行胶片测量和计算时,局部高剂量差异(>4%)的区域在使用三个孔径进行计算时显著减少。电离室测量也显示了类似的结果,使用额外孔径进行计算时有所改进。通过开发一种射束注量矩阵的采样方法,TG建模的剂量计算精度进一步提高。对于我们分辨率为1mm的注量矩阵,通过MLC传输的注量采用单元素点采样。对于瓦里安HDMLC,栅格对准会导致注量采样误差。为了纠正这一点,应用了传输体积平均法。对于三个脊柱旁HDMLC病例,在胶片和计算比较中,采用我们的新方法时平均剂量差异大大降低。对于三个病例,在不进行体积平均的计算和进行体积平均的计算中,伽马(3%,3mm)通过率分别从74.1%、90.0%和90.4%显著提高到99.2%、97.9%和97.3%。我们的结果表明,更精确的MLC叶片位置和传输采样可以提高计算与测量之间的准确性和一致性,对于由大MLC运动组成的大分割VMAT尤为重要。