Warren Samantha, Partridge Mike, Bolsi Alessandra, Lomax Anthony J, Hurt Chris, Crosby Thomas, Hawkins Maria A
Cancer Research UK/Medical Research Council Oxford Institute for Radiation Oncology, Gray Laboratories, University of Oxford, Oxford, United Kingdom.
Cancer Research UK/Medical Research Council Oxford Institute for Radiation Oncology, Gray Laboratories, University of Oxford, Oxford, United Kingdom.
Int J Radiat Oncol Biol Phys. 2016 May 1;95(1):199-207. doi: 10.1016/j.ijrobp.2016.01.044. Epub 2016 Jan 30.
Planning studies to compare x-ray and proton techniques and to select the most suitable technique for each patient have been hampered by the nonequivalence of several aspects of treatment planning and delivery. A fair comparison should compare similarly advanced delivery techniques from current clinical practice and also assess the robustness of each technique. The present study therefore compared volumetric modulated arc therapy (VMAT) and single-field optimization (SFO) spot scanning proton therapy plans created using a simultaneous integrated boost (SIB) for dose escalation in midesophageal cancer and analyzed the effect of setup and range uncertainties on these plans.
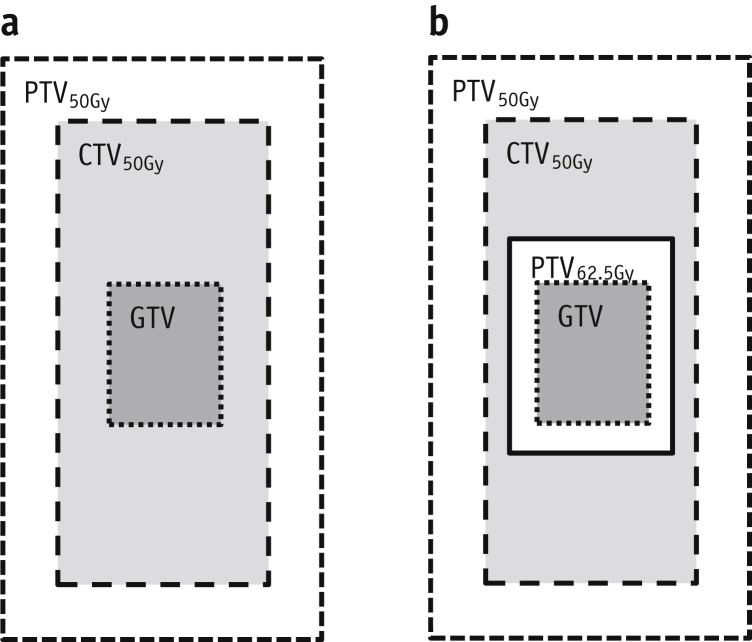
For 21 patients, SIB plans with a physical dose prescription of 2 Gy or 2.5 Gy/fraction in 25 fractions to planning target volume (PTV)50Gy or PTV62.5Gy (primary tumor with 0.5 cm margins) were created and evaluated for robustness to random setup errors and proton range errors. Dose-volume metrics were compared for the optimal and uncertainty plans, with P<.05 (Wilcoxon) considered significant.
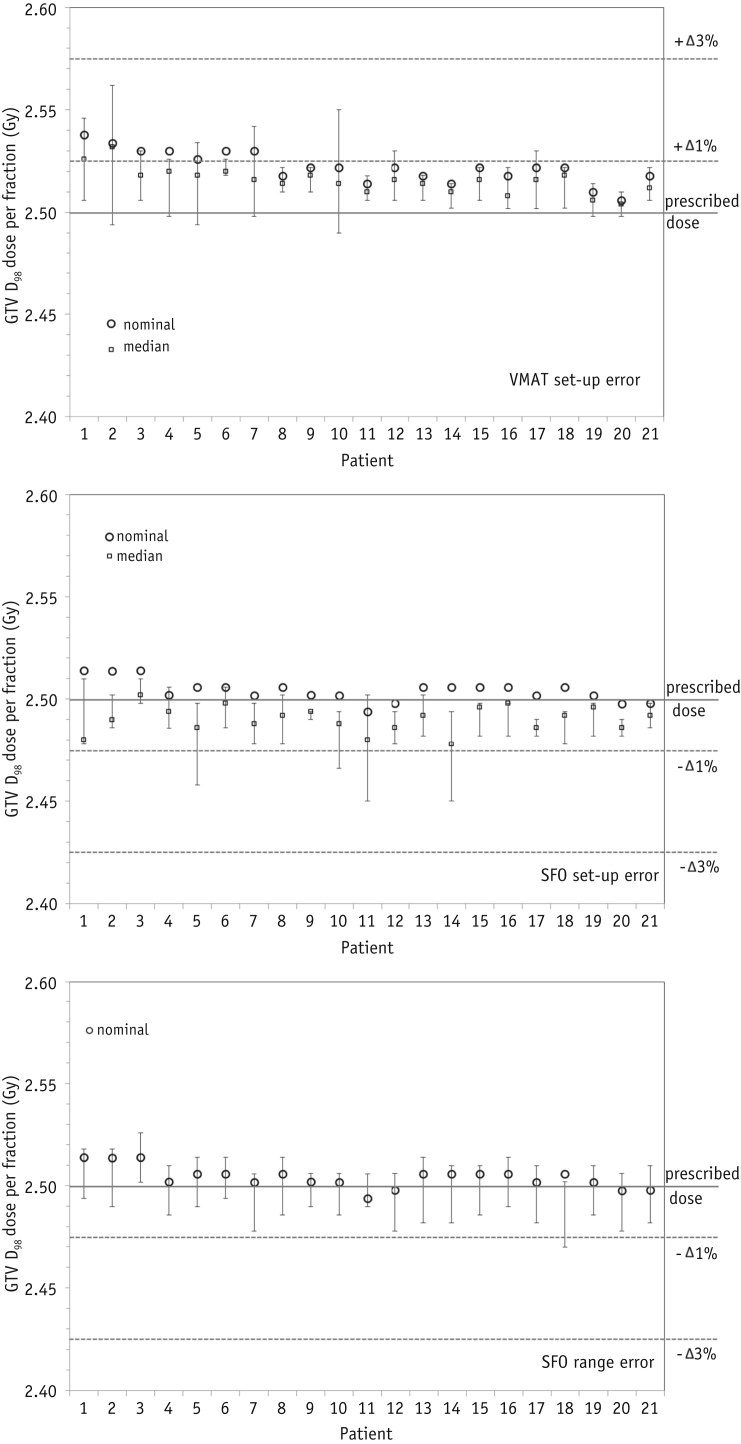
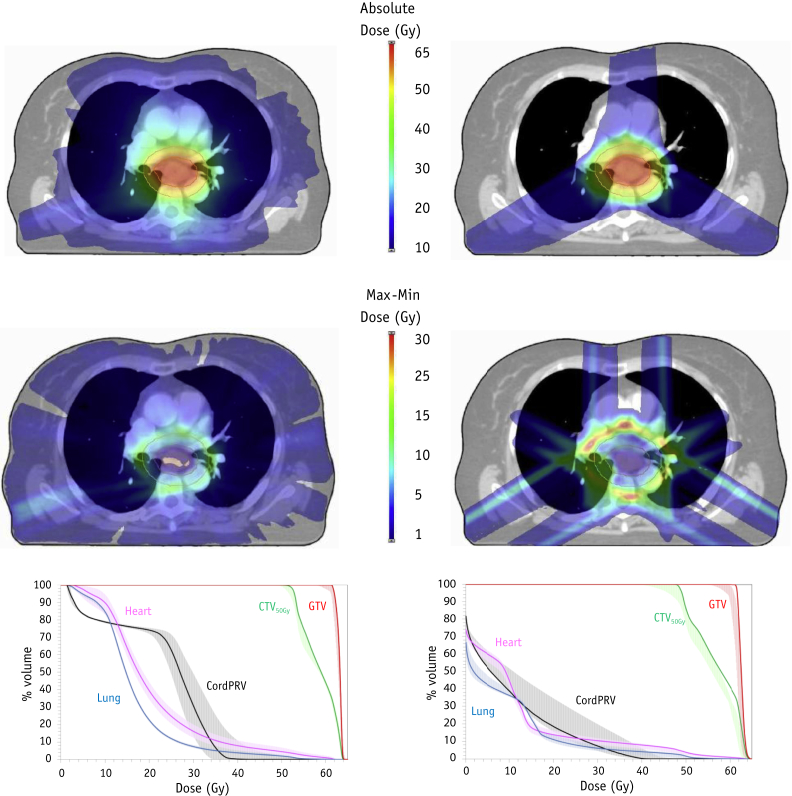
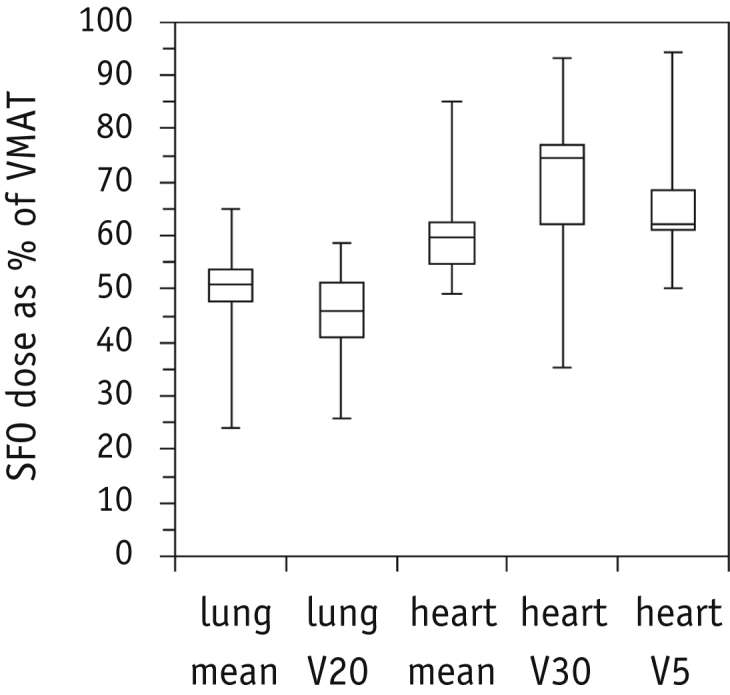
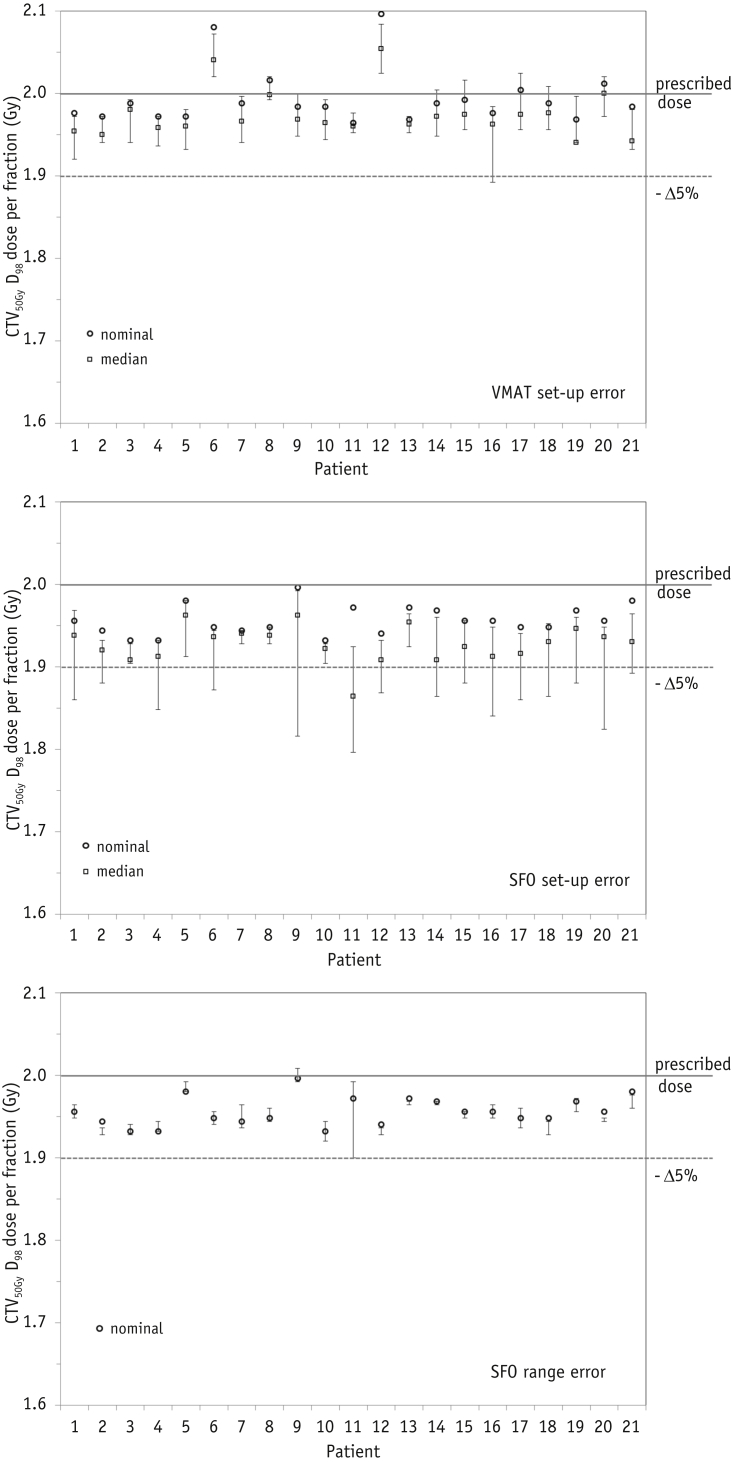
SFO reduced the mean lung dose by 51.4% (range 35.1%-76.1%) and the mean heart dose by 40.9% (range 15.0%-57.4%) compared with VMAT. Proton plan robustness to a 3.5% range error was acceptable. For all patients, the clinical target volume D98 was 95.0% to 100.4% of the prescribed dose and gross tumor volume (GTV) D98 was 98.8% to 101%. Setup error robustness was patient anatomy dependent, and the potential minimum dose per fraction was always lower with SFO than with VMAT. The clinical target volume D98 was lower by 0.6% to 7.8% of the prescribed dose, and the GTV D98 was lower by 0.3% to 2.2% of the prescribed GTV dose.
The SFO plans achieved significant sparing of normal tissue compared with the VMAT plans for midesophageal cancer. The target dose coverage in the SIB proton plans was less robust to random setup errors and might be unacceptable for certain patients. Robust optimization to ensure adequate target coverage of SIB proton plans might be beneficial.
比较X射线和质子技术并为每位患者选择最合适技术的规划研究,因治疗计划和实施的几个方面不相等而受到阻碍。公平的比较应比较当前临床实践中同样先进的实施技术,并评估每种技术的稳健性。因此,本研究比较了使用同步整合加量(SIB)进行中食管癌剂量递增时,容积调强弧形放疗(VMAT)和单野优化(SFO)点扫描质子治疗计划,并分析了摆位和射程不确定性对这些计划的影响。
对21例患者,制定了物理剂量处方为2Gy或2.5Gy/分次、共25分次至计划靶体积(PTV)50Gy或PTV62.5Gy(原发肿瘤外放0.5cm边界)的SIB计划,并评估其对随机摆位误差和质子射程误差的稳健性。比较了最优计划和不确定性计划的剂量体积指标,P<0.05(Wilcoxon检验)认为有统计学意义。
与VMAT相比,SFO使平均肺剂量降低了51.4%(范围35.1%-76.1%),平均心脏剂量降低了40.9%(范围15.0%-57.4%)。质子计划对3.5%射程误差的稳健性是可接受的。对所有患者,临床靶体积D98为处方剂量的95.0%至100.4%,大体肿瘤体积(GTV)D98为98.8%至101%。摆位误差稳健性取决于患者解剖结构,且SFO每次分次的潜在最小剂量始终低于VMAT。临床靶体积D98比处方剂量低0.6%至7.8%,GTV D98比处方GTV剂量低0.3%至2.2%。
对于中食管癌,与VMAT计划相比,SFO计划显著减少了正常组织受量。SIB质子计划中的靶区剂量覆盖对随机摆位误差的稳健性较差,对某些患者可能不可接受。进行稳健优化以确保SIB质子计划有足够的靶区覆盖可能是有益的。