Lee Taebum, Lee Boram, Choi Yoon-La, Han Joungho, Ahn Myung-Ju, Um Sang-Won
Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
J Pathol Transl Med. 2016 May;50(3):197-203. doi: 10.4132/jptm.2016.03.09. Epub 2016 Apr 18.
Although epidermal growth factor receptor (EGFR), v-Ki-ras2 Kirsten rat sarcoma viral oncogene (KRAS), and anaplastic lymphoma kinase (ALK) mutations in non-small cell lung cancer (NSCLC) were thought to be mutually exclusive, some tumors harbor concomitant mutations. Discovering a driver mutation on the basis of morphologic features and therapeutic responses with mutation analysis can be used to understand pathogenesis and predict resistance in targeted therapy.
In 6,637 patients with NSCLC, 12 patients who had concomitant mutations were selected and clinicopathologic features were reviewed. Clinical characteristics included sex, age, smoking history, previous treatment, and targeted therapy with response and disease-free survival. Histologic features included dominant patterns, nuclear and cytoplasmic features.
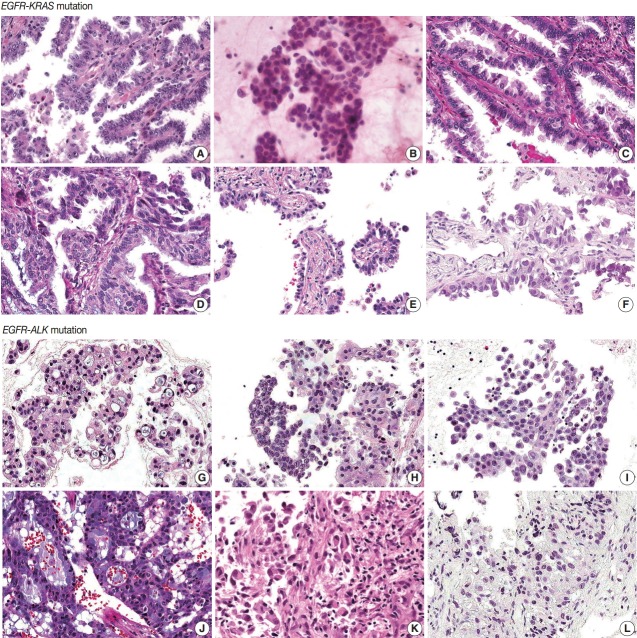
All patients were diagnosed with adenocarcinoma and had an EGFR mutation. Six patients had concomitant KRAS mutations and the other six had KRAS mutations. Five of six EGFR-KRAS mutation patients showed papillary and acinar histologic patterns with hobnail cells. Three of six received EGFR tyrosine kinase inhibitor (TKI) and showed partial response for 7-29 months. All six EGFR-ALK mutation patients showed solid or cribriform patterns and three had signet ring cells. Five of six EGFR-ALK mutation patients received EGFR TKI and/or ALK inhibitor and four showed partial response or stable disease, except for one patient who had acquired an EGFR mutation.
EGFR and ALK mutations play an important role as driver mutations in double mutated NSCLC, and morphologic analysis can be used to predict treatment response.
虽然非小细胞肺癌(NSCLC)中的表皮生长因子受体(EGFR)、v-Ki-ras2 Kirsten大鼠肉瘤病毒致癌基因(KRAS)和间变性淋巴瘤激酶(ALK)突变被认为是相互排斥的,但一些肿瘤存在伴随突变。基于形态学特征和突变分析的治疗反应发现驱动突变可用于理解发病机制并预测靶向治疗中的耐药性。
在6637例NSCLC患者中,选择12例有伴随突变的患者并回顾其临床病理特征。临床特征包括性别、年龄、吸烟史、既往治疗以及靶向治疗的反应和无病生存期。组织学特征包括主要模式、细胞核和细胞质特征。
所有患者均被诊断为腺癌且有EGFR突变。6例患者有KRAS伴随突变,另外6例有ALK突变。6例EGFR-KRAS突变患者中有5例表现为伴有鞋钉样细胞的乳头状和腺泡状组织学模式。6例中有3例接受了EGFR酪氨酸激酶抑制剂(TKI)治疗并显示7至29个月的部分缓解。所有6例EGFR-ALK突变患者均表现为实性或筛状模式,3例有印戒细胞。6例EGFR-ALK突变患者中有5例接受了EGFR TKI和/或ALK抑制剂治疗,除1例获得EGFR突变的患者外,4例显示部分缓解或病情稳定。
EGFR和ALK突变在双突变NSCLC中作为驱动突变发挥重要作用,形态学分析可用于预测治疗反应。