Robinson Mark W, Hughes Joseph, Wilkie Gavin S, Swann Rachael, Barclay Stephen T, Mills Peter R, Patel Arvind H, Thomson Emma C, McLauchlan John
MRC - University of Glasgow Centre for Virus Research, Institute of Infection, Immunity and Inflammation, University of Glasgow, Glasgow, UK; School of Biochemistry and Immunology, Trinity Biomedical Sciences Institute, Trinity College Dublin, Dublin, Ireland.
MRC - University of Glasgow Centre for Virus Research, Institute of Infection, Immunity and Inflammation, University of Glasgow , Glasgow , UK.
Front Immunol. 2016 Apr 5;7:131. doi: 10.3389/fimmu.2016.00131. eCollection 2016.
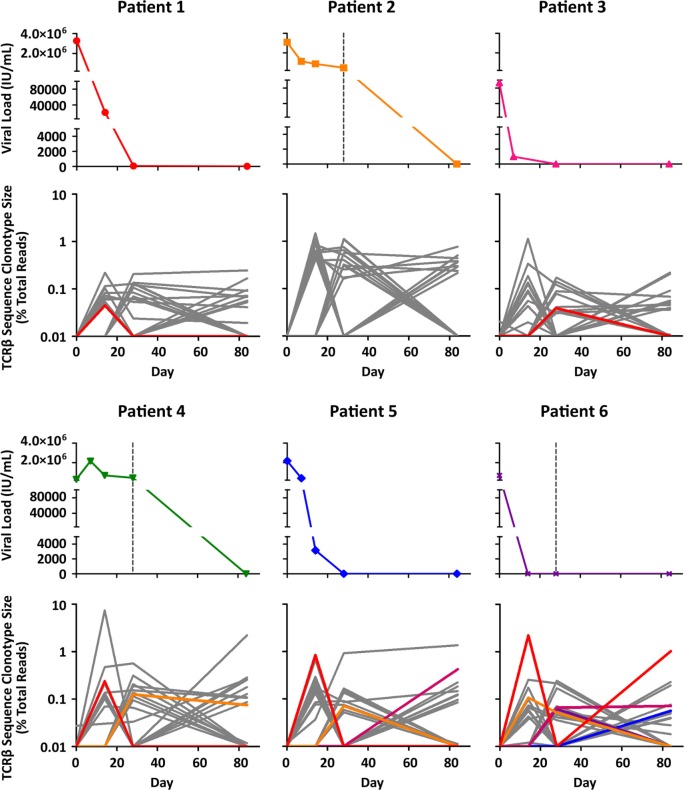
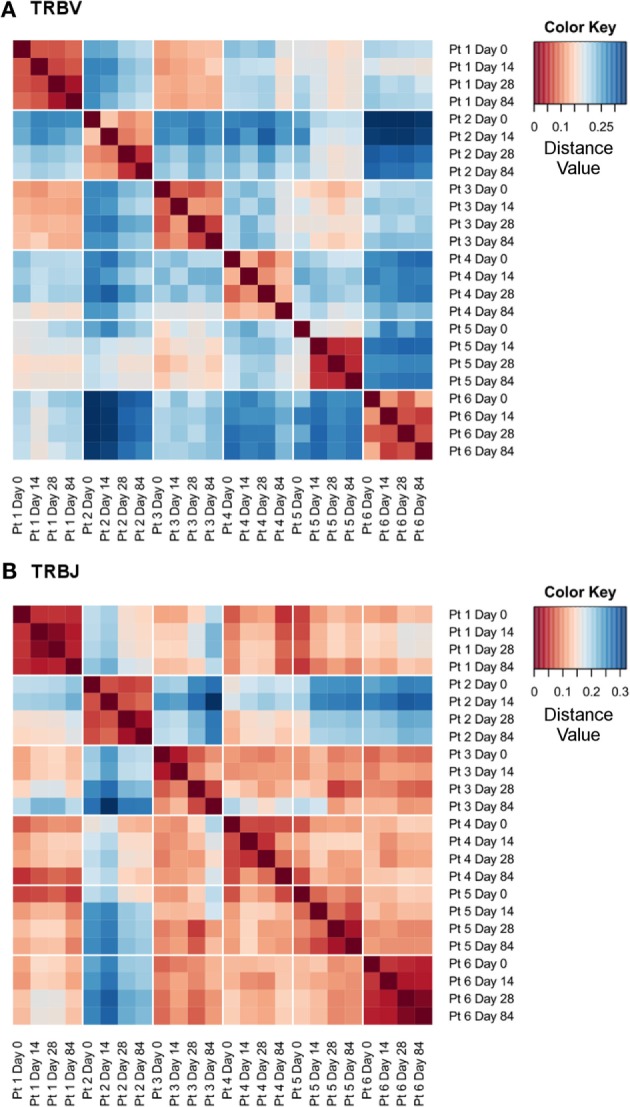
To maintain a persistent infection viruses such as hepatitis C virus (HCV) employ a range of mechanisms that subvert protective T cell responses. The suppression of antigen-specific T cell responses by HCV hinders efforts to profile T cell responses during chronic infection and antiviral therapy. Conventional methods of detecting antigen-specific T cells utilize either antigen stimulation (e.g., ELISpot, proliferation assays, cytokine production) or antigen-loaded tetramer staining. This limits the ability to profile T cell responses during chronic infection due to suppressed effector function and the requirement for prior knowledge of antigenic viral peptide sequences. Recently, high-throughput sequencing (HTS) technologies have been developed for the analysis of T cell repertoires. In the present study, we have assessed the feasibility of HTS of the TCRβ complementarity determining region (CDR)3 to track T cell expansions in an antigen-independent manner. Using sequential blood samples from HCV-infected individuals undergoing antiviral therapy, we were able to measure the population frequencies of >35,000 TCRβ sequence clonotypes in each individual over the course of 12 weeks. TRBV/TRBJ gene segment usage varied markedly between individuals but remained relatively constant within individuals across the course of therapy. Despite this stable TRBV/TRBJ gene segment usage, a number of TCRβ sequence clonotypes showed dramatic changes in read frequency. These changes could not be linked to therapy outcomes in the present study; however, the TCRβ CDR3 sequences with the largest fold changes did include sequences with identical TRBV/TRBJ gene segment usage and high junction region homology to previously published CDR3 sequences from HCV-specific T cells targeting the HLA-B0801-restricted (1395)HSKKKCDEL(1403) and HLA-A0101-restricted (1435)ATDALMTGY(1443) epitopes. The pipeline developed in this proof of concept study provides a platform for the design of future experiments to accurately address the question of whether T cell responses contribute to SVR upon antiviral therapy. This pipeline represents a novel technique to analyze T cell dynamics in situations where conventional antigen-dependent methods are limited due to suppression of T cell functions and highly diverse antigenic sequences.
为维持持续性感染,丙型肝炎病毒(HCV)等病毒会采用一系列破坏保护性T细胞反应的机制。HCV对抗原特异性T细胞反应的抑制阻碍了在慢性感染和抗病毒治疗期间分析T细胞反应的工作。检测抗原特异性T细胞的传统方法要么利用抗原刺激(如酶联免疫斑点法、增殖试验、细胞因子产生),要么利用负载抗原的四聚体染色。由于效应功能受到抑制以及需要事先了解抗原性病毒肽序列,这限制了在慢性感染期间分析T细胞反应的能力。最近,已开发出高通量测序(HTS)技术用于分析T细胞库。在本研究中,我们评估了对TCRβ互补决定区(CDR)3进行HTS以抗原非依赖方式追踪T细胞扩增的可行性。利用接受抗病毒治疗的HCV感染者的连续血样,我们能够在12周的过程中测量每个个体中超过35,000种TCRβ序列克隆型的群体频率。TRBV/TRBJ基因片段的使用在个体之间有显著差异,但在治疗过程中个体内部保持相对稳定。尽管TRBV/TRBJ基因片段的使用稳定,但一些TCRβ序列克隆型的读取频率显示出显著变化。在本研究中,这些变化与治疗结果无关;然而,变化倍数最大的TCRβ CDR3序列确实包括与先前发表的针对HLA - B0801限制性(1395)HSKKKCDEL(1403)和HLA - A0101限制性(1435)ATDALMTGY(1443)表位的HCV特异性T细胞的CDR3序列具有相同TRBV/TRBJ基因片段使用和高连接区同源性的序列。在这个概念验证研究中开发的流程为设计未来实验提供了一个平台,以准确解决抗病毒治疗后T细胞反应是否有助于实现持续病毒学应答(SVR)的问题。该流程代表了一种新技术,用于在传统的抗原依赖方法由于T细胞功能抑制和高度多样的抗原序列而受到限制的情况下分析T细胞动态。