Hatemi Ibrahim, Esatoglu Sinem Nihal, Hatemi Gulen, Erzin Yusuf, Yazici Hasan, Celik Aykut Ferhat
From the Division of Gastroenterology, Department of Internal Medicine (IH, YE, AFC), Cerrahpasa Medical School, Istanbul University, Istanbul, Turkey; and Division of Rheumatology (SNE GH, HY), Department of Internal Medicine, Cerrahpasa Medical School, Istanbul University, Istanbul, Turkey.
Medicine (Baltimore). 2016 Apr;95(16):e3348. doi: 10.1097/MD.0000000000003348.
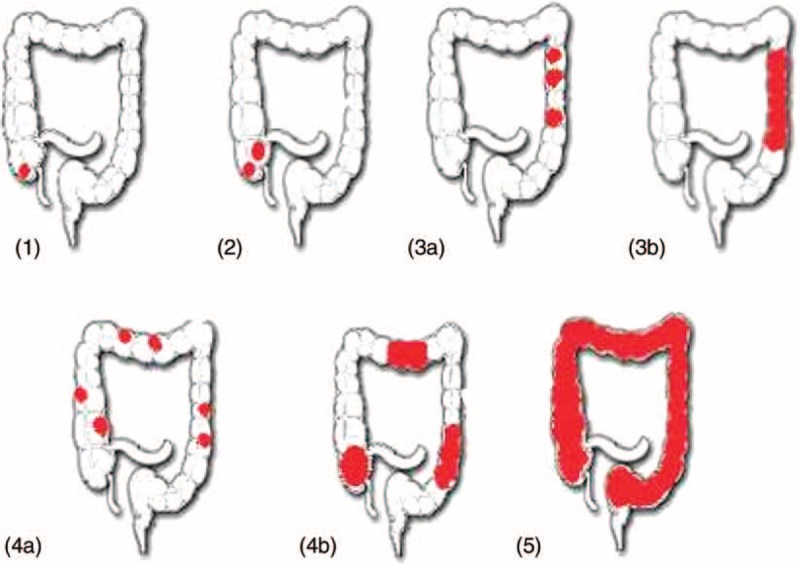
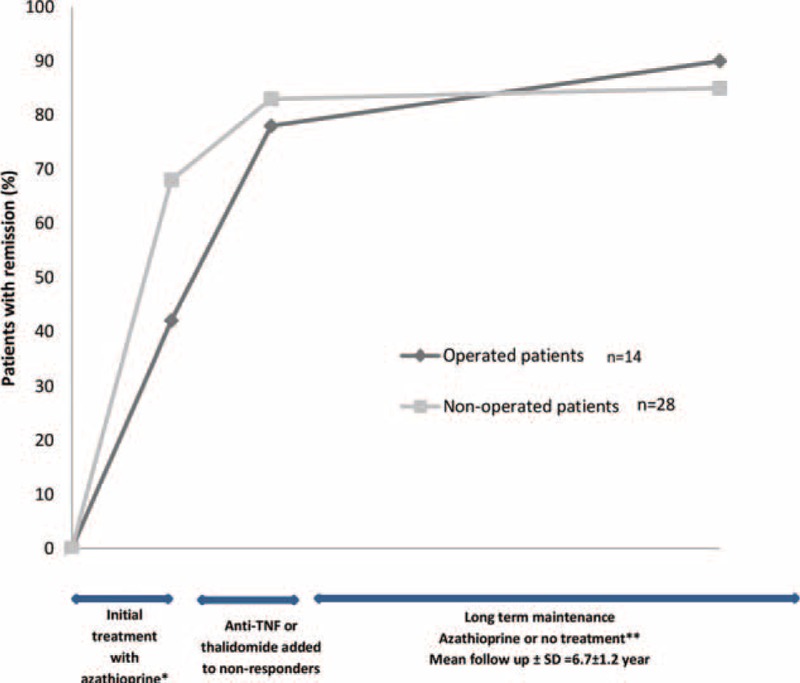
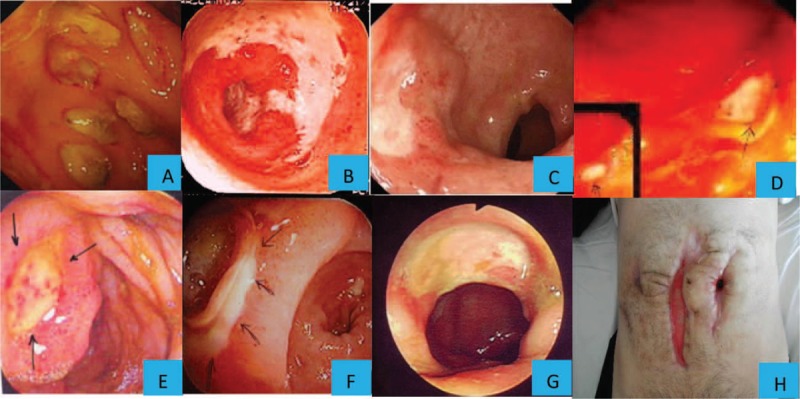
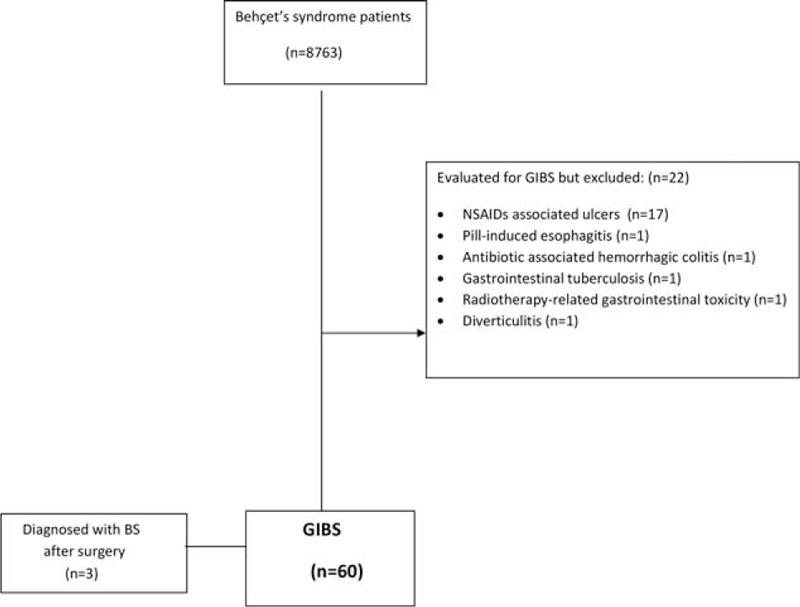
Gastrointestinal involvement is rare in Behçet's syndrome (BS) patients from the Mediterranean basin. We report the demographic and disease characteristics, treatment modalities, and outcome of patients with gastrointestinal involvement in BS (GIBS). We retrospectively reviewed the charts of all BS patients in our BS clinic with a diagnosis of GIBS. Patients were invited to the clinic to assess their outcome. Among 8763 BS patients, we identified 60 with GIBS (M/F: 32/28, mean age at diagnosis: 34 ± 10, mean follow-up: 7.5 ± 4 years), after excluding 22 patients with mimicking symptoms. Six (10%) had juvenile-onset BS. The most common intestinal localization was ileocecal region (36/59, 61%) mainly as big oval ulcer/s. Initial treatment was azathioprine for moderate to severe (n = 37) and 5-ASA for mild cases (n = 16). Anti-TNFs and/or thalidomide provided remission in 12 of 18 (67%) refractory patients. Emergency surgery was required in 22 patients. Nine patients did not receive postoperative immunomodulators and 8 relapsed. Overall, 48 of 60 (80%) patients were in remission (29/48 without treatment) at the time of survey. Three recently treated and 2 refractory patients were still active, 3 had died due to non-GI-related reasons, and 4 were lost to follow-up. Careful evaluation for excluding mimickers is important during the diagnosis of GIBS. Azathioprine seems to be a good choice as first-line treatment with high remission rates and few adverse events. Thalidomide and/or TNF-alpha antagonists may be preferred in resistant cases. Surgery may be required for perforations or massive bleeding, and postoperative immunosuppressive treatment is necessary for preventing postoperative recurrences.
在地中海地区的白塞病(BS)患者中,胃肠道受累情况较为罕见。我们报告了白塞病胃肠道受累患者(GIBS)的人口统计学和疾病特征、治疗方式及预后情况。我们回顾性分析了我院白塞病门诊所有诊断为GIBS患者的病历。邀请患者到门诊评估其预后。在8763例BS患者中,排除22例有类似症状的患者后,我们确定了60例GIBS患者(男/女:32/28,诊断时平均年龄:34±10岁,平均随访时间:7.5±4年)。其中6例(10%)为青少年起病的BS。最常见的肠道病变部位是回盲部(36/59,61%),主要表现为大的椭圆形溃疡。初始治疗中,中度至重度患者(n = 37)使用硫唑嘌呤,轻度患者(n = 16)使用5-氨基水杨酸。18例难治性患者中有12例(67%)使用抗TNF药物和/或沙利度胺后病情缓解。22例患者需要急诊手术。9例患者术后未接受免疫调节剂治疗,8例复发。总体而言,在调查时,60例患者中有48例(80%)病情缓解(其中29例未接受治疗)。3例近期接受治疗的患者和2例难治性患者病情仍未缓解,3例因非胃肠道相关原因死亡,4例失访。在GIBS诊断过程中,仔细评估以排除疑似病例很重要。硫唑嘌呤似乎是一线治疗的良好选择,缓解率高且不良事件少。在耐药病例中,可优先选择沙利度胺和/或TNF-α拮抗剂。对于穿孔或大量出血可能需要手术治疗,术后免疫抑制治疗对于预防术后复发是必要的。